Home » Posts tagged 'research'
Tag Archives: research
Cut and Paste vs the Computer
 Around 2011 during the Master of Arts Open & Distance Education I resolved to give up on paper entirely: no files, no printing off and all books on Kindle. This time round I stay off the computer except for wordpressing, posting essays and supervisor feedback. Instead I am back to my teen student days of pen, paper, scissors and Sellotape and large scraps of coloured paper. It works for me, even if it is somewhat time consuming.
Around 2011 during the Master of Arts Open & Distance Education I resolved to give up on paper entirely: no files, no printing off and all books on Kindle. This time round I stay off the computer except for wordpressing, posting essays and supervisor feedback. Instead I am back to my teen student days of pen, paper, scissors and Sellotape and large scraps of coloured paper. It works for me, even if it is somewhat time consuming.
What I haven’t understood is that greater academic skill at taking notes from references would greatly reduce the need to compost, then filter down a mass of too much information at a later date.
Getting there. This 15,000 word dissertation on the behaviour and mood of volunteers as they enlisted in early September 1914 is not due until July.
From time to time I am faced with finding the most obscure of articles
 |
| From First World War |
Fig.1 Motorbike Ambulance of the First World War
I came across something about the Ambulance Service using motorbikes during the First World War. I then saw a photograph of a motorbike with a sidecar with a set of platforms that would carry two stretchers. The arguments for the use of a motorcycle are made: lighter, quicker, tighter turning circle, use less fuel …
A article is cited. The British Medical Journal, January 1915. A few minutes later via the Open University Online Library I locate and download the article.
It is the speed at which quality research can be fulfilled that thrills me. This article is satisfying in its own right, but glancing at the dozen or more articles on medical practices and lessons from the Front Line are remarkable. We are constantly saved from the detail of that conflict, the stories and issues regurgitated and revisited as historians read what previous historians said without going back to the original source.
This is how a new generation can come up with a fresh perspective on the First World War – instead of a handful of specialist academics burrowing in the paper archives now thousands, even tens of thousands can drill right down to the most pertinent, untampered with content.
 |
| From First World War |
Amazed.
Why most published research findings are false
Why most published research findings are false
REFERENCE
Ioannidis, J A 2005, ‘Why Most Published Research Findings Are False’, Plos Medicine, 2, 8, pp. 696-701, Academic Search Complete, EBSCOhost, viewed 12 February 2013.
Writers have the details at their fingertips
 |
| From E-Learning V |
Fig.1 Moon phases in May 1917
Studying with the OU for the last four years it soon become natural to conduct online niche searches for books and papers related to course work. You learn also how to tag, store and gather the information and ideas that you find: this is one answer to that, a blog that serves several purposes, not least as a learning journal and e-portfolio.
Searching for the obscure, that essential detail that forms such a vital part of the sensory palette used by the writer, is as easy to find and just as necessary. This morning I stepped out one May evening in 1917 and wanted some hint of what I’d see, hear and feel: a few searches and I can see a waxing moon at 10.00pm on a cooling evening as the temperature dips below 12 degree C, and the noise, in this instance of thousands of men in Nissen huts around a camp soon giving way to a robin trilling and burbling in the trees and the sound of the sea washing against the Channel Coast.
These details are far more than accessories that overlay character and plot; they are what gives it credibility. Writing on and as the Great War rages requires significant care. The wrong detail will throw a reader, worse I’ll end up in a conversation about my claims. Posting a piece of fiction some years ago an irate reader told me what I’d said was rot and went on to correct me – I had been writing fiction. I’d said that a character called Gustav Hemmel changed his name to George Hepple and fakes his own death – the reality is that he went missing over the English Channel in his plane.
THREE HOURS working on writing fiction, five days a week, is the goal . The OU will have me for TWO hours a day (averaged with longer stints at the weekend). That’s the plan.
Can an email-prompted web-based e-learning platform aimed at undergraduates in the UK with moderate to persistent asthma improve compliance to their prescribed preventer drugs to 80%?

Fig. 1 Preventer, Reliever and volumetric. With good adherence the ‘brown one’ is taken as prescribed and the ‘blue one’ rarely needed. With poor adherence there is no brown on and there is dependence on the blue one. In this example a QVAR easibreather and a Venotlin inhaler. Mine.
By presenting these ideas here I asking for support on how to make this research happen.
The medical profession is replacing the term ‘adherence’ with the term ‘compliance’. This reflects the desire to encourage self-management of prescribed drugs in concordance with health care providers (HCPs). For the purposes of this paper the terms should be considered interchangeable.
Asthma is a chronic and complex condition affecting the lungs that can be managed but not cured. (NHS Choices, 2013) (See Appendix 1 for a definition of ‘moderate to persistent asthma’). The World Health Organisation estimates that 300 million people globally are asthmatic (Web, 2001) while in the UK in 2010 5.4 million people were receiving treatment for asthma and there were 1,143 deaths. (Asthma, UK. 2013) An estimated 75% of hospital admissions for asthma are avoidable and as many as 90% of the deaths are preventable. (Asthma, UK. 2013) 80% compliance is the minimal level required for treatment to be effective (Lasmar et al., 2009).
Research construct
Asthmatics form a heterogeneous group that shows great diversity of triggers, effective medication, management strategies and outcomes. Research clusters asthmatics into four to six groups based on how they present and the drug regime they are on (Webb, 2011). Isolating a participant’s conditions and being confident that their medication is correct will be a challenge. For this reason, thorough in-depth interviews with participants, potentially with an HCP present, will be vital in order to set a benchmark.
A team at Harvard Medical School designed Qstream, the proposed e-learning platform (Kerfoot et al., 2008). Qstream (Fig.1.) takes its approach from an understanding of Ebbinghaus (Ebbinghaus, 1913) and how we forget and remember to provide a spaced-learning response that uses a combination of email alerts and interactive content to build knowledge. Its use has been researched with junior doctors in relation to their formal medical training and assessment (Kerfoot et al., 2008; Kerfoot et al., 2012) and in applied settings with healthcare practitioners to support informed decision-making. (Kerfoot et al., 2010)
Fig.1. Screengrab from Qstream homepage. (www.qstream.com)
On the basis of their research, Dr B Price Kerfoot says that ‘educational games work’ (Kerfoot et al., 2008. Kerfoot suggests that the next step is to use this approach with patients and ‘clinical decisions of greater complexity’ Kerfoot (2010:477). Research using Qstream involving people with chronic illnesses is planned to take place in North America in the Fall of 2013 (Vernon and Kerfoot, 2013).
What is the problem?
Too many people with a chronic illness, such as asthma, fail to take their medication as prescribed (Royal Pharmaceutical Society (RPS) of Great Britain, 1997; Hayes et al., 1979). This can lead to an exacerbation of the disease, risks hospitalization and even death. Non-compliancy rates are between 10-60% (Cochrane, 1992. Rand,1994), 30–50% (Horne, 1999), 50% (Di Matteo, Giordani, Lepper & Croghan, 2001; Kyngas, 2007 in Wales et al., 2011:148).
Reasons for non-compliance include medication side effects, expense of treatment, personal value judgments or religious or cultural beliefs about the proposed treatment, age–related debility, not having an action plan prescribed by an HCP, the patient not following the adequate treatment prescribed (Cerveri et al., (1999:288) or the presence of a mental disorder (e.g., schizophrenia, personality disorder). American Psychiatric Association [DSM-5], (2013:726).
What is the opportunity?
According to McGavock et al., (1996) efforts to improve compliance have been unsuccessful; it is hoped that efforts using e-learning will be successful. The healthcare community – manufacturers, prescribers and frontline carers, recognise that education offers a way to reduce hospital admissions and deaths (Cerveri et al.,1999:288). The opportunity exists to increase compliance to 80% and therefore improve the health of millions of people with asthma.
A variety of programmes have tested a potential solution to non-adherence. (Byer & Myers, 2000; Hand, 1998; Tettersell, 1993), while Hacihasanoğlu and Goözuöm (2011) showed that patient education on medication adherence is effective. A variety of studies on e-learning in healthcare have used emails linked to multiple-choice questions and answers to improve patients’ knowledge and behaviours (Volpp et al. 2009; Kato et al. 2008).
The hypothesis
The hypothesis is that as a result of greater compliance through a ‘spaced learning’ e-learning education programme, non-compliant moderately persistent asthmatics will show changes in measurements of their illness and changes in their medication beliefs. (Based on Petrie et al., 2012:76).
Desired outcomes / results
Having completed a programme of e-learning using Qstream people with moderate to persistent asthma who had been noncompliant (under 80% compliant) should show changes in their illness and medication beliefs, improved compliance to their preventer inhaler and measured improvement across a range of physiological measures. (Based on Petrie et al., 2012:76) As a result of what they learn, the research will address patient perceptions, such as beliefs (Horne & Weinman, 2002), worries about long term use of steroids (Apter et al., 2003), fears and other concerns (Kaptein, Klok, Moss-Morrs & Brand, 2010). For example, 28% of asthma patients think that drugs are bad and not necessary while 12% think that drugs may not be not bad but aren’t necessary. Cerveri et al., (1999:292).
Achieving a reasonable level of compliance with treatment regimes has been shown to improve the health outcomes of patients undergoing treatment and reduce demands on health resources (Bender, Milgrom, Wamboldt & Rand, 2000; Dunbar-Jacob, Burke & Puczynski, 1995).
The long-term and broader opportunity exists to reduce hospitalizations, reduce costs, improve and extend lives.
Learning Theories
The learning theories that form the basis of Qstream are behaviourist (Skinner, 1974) and cognitive (Wenger, 1987; Hutchins, 1993; Anderson, 1983; Piaget, 1952) with problem solving, explanations and re-combinations. In line with this behaviourist approach early versions of Qstream worked best in formal learning contexts, for example first year medical students needing to pass an exam on anatomy. (Kerfoot et al., 2008) and practical clinical guidelines (Kerfoot et al., 2009). By complementing traditional medical training, with clear goals and the motivation to pass, the attraction of the platform are clear in this context. This stimulus-response approach, builds on the work of Ebbinghaus (1913) (Fig. 2)
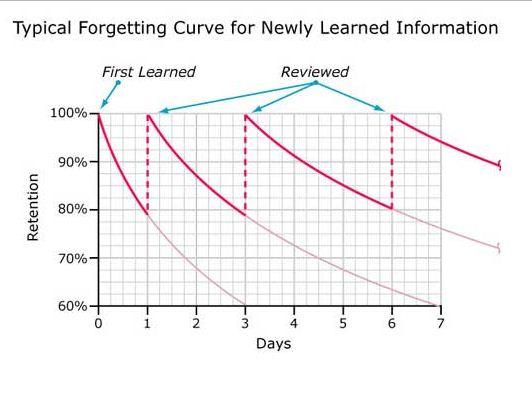
Fig. 2. A typical forgetting curve for newly learned information. After Ebbinghaus (1913)
Through association, the learner takes a number of steps to build a composite skill. (Skinner, 1984; Gagné, 1985) (Fig.3) An accurate reproduction of knowledge can be assessed or demonstrated in drill and practice.
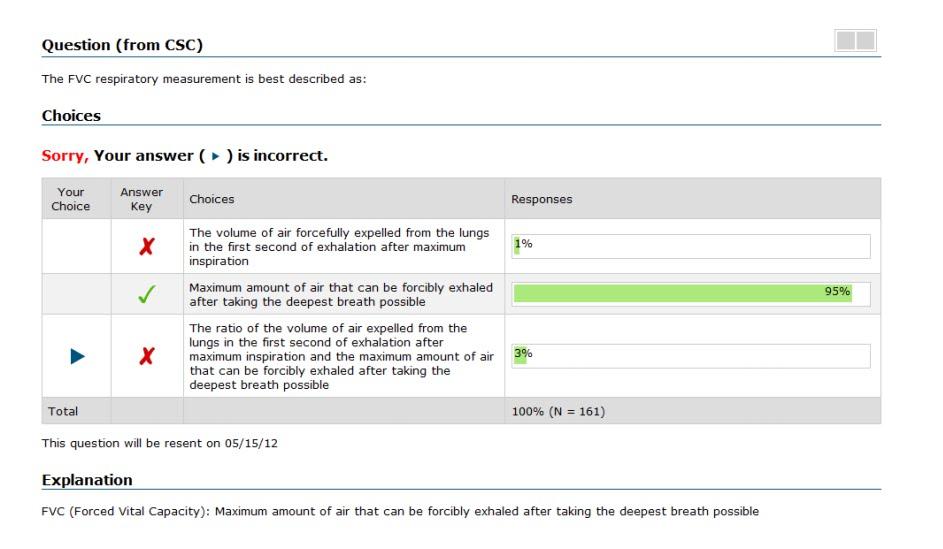
Fig.3. Screengrab from Qstream showing how a participant receives feedback on their response to a multiple-choice question.
Later and current versions of Qstream include components of peer competition, participant interaction and collaboration. This constructivist approach takes the view that learners build their own structures (Piaget, 1954). It also suites task orientated learning (Bruner, 1993) and assimilative learning. This constructed and socio-constructed approach to learning is less suited to assessment simply by looking at exam grades, therefore in-depth interviews or comprehensive self-reporting surveys are required to elicit what took place and the level of knowledge attained especially as evidence of learning by people with asthma won’t be elicited through formal assessment.
Why undergraduates?
The research shows that younger asthma patients in the age 14-25 years are less likely to use their preventer medication than older patients (Diette et al., 1999; Legorreta et al., 1998), which makes ‘young people an important group to target for improving adherence and reducing their underuse of preventer-inhaler corticosteroids’, (Pertie et al., 2012:75). For this reason, and to exploit study parameters of population size and geography, a university undergraduate population is proposed.
METHODOLOGY/METHODS
A mixed-method approach will be adopted with qualitative and quantitative components. In-depth pre and post intervention interviews will form the qualitative element, while the quantitative component will be based on several hundred student participants taking part in a randomized controlled trial and use analytics generated by the Qstream platform. The aim is to interview approximately 30 students in-depth within the parameters of a single university. For example, Adams, Pill & Jones, (1997) favoured in depth interviews with a carefully selected and eligible number of patients before and after intervention. For quantitative analysis the far larger pool of participants will be drawn from a UK wide undergraduate student population using platforms such as The Student Room (www.thestudentroom.com. The Student Room, 2013) and Asthma UK to recruit participants. According to Kerfoot & Baker (2012) an individual randomized control trial is preferable were there is a large sample size. Extending to a sample of four UK universities might increase the potential number of participants to 9000+ (See Appendix 2). Self-reporting screening would be used to ensure that only those in the desired group took part.
Based on UK statistics on asthma in the population, it can be calculated that at, for example, the University of Southampton from a total undergraduate population of 17,000 there are likely to be between 485 and 586 students with moderate to severe asthma. (This intentionally excludes those likely to have a mild form of the disease, and those with a profoundly severe form of the condition). (See Appendix 2 for break down of likely respondents). Asthma UK (2013) suggests that amongst asthmatics 48% consider themselves to be at risk. If this percentage of potential participants volunteered then the starting population for the proposed research is likely to be around 250. It is reasonable to suggest that by working with four different universities of a similar size the total population for a randomized control trial would increase to 1,000.
Identifying those who are moderate to severe asthmatics and agreeing criteria has confounded asthma studies in the past, therefore great care will be required to set parameters, the simplest being that where an asthmatic has been prescribed only two medications, a preventer inhaler (known as the ‘brown one’) and the reliever inhaler (the ‘blue one’) that their condition is considered to be ‘moderate to severe’.
Having a sound basis for giving a person’s baseline, for both compliance and knowledge of asthma and how it is treated, will indicate if an improvement in adherence has been made and whether this e-learning approach has been effective.
To have a physical measure you can audit the prescriptions issued or weigh the inhalers to establish how much has been expelled, however Spector (1985) found cases of both miss-application and trial firing. A blood test is definitive, but this could only be carried out by an HCP. The alternative is to ask patients how they got on, however patients are thought to overestimate their actual drug use by between 30 and 50% (Spector, 1985; Sacket and Snow, 1979). In the case of people with asthma, Horn (1992:126) found that 11% who claimed to have inhaled salbutamol in the preceding four hours had no detectable drug in their urine.
Whilst therefore there are advantages in conducting interviews, patients are giving a subjective measure of their treatment compliance (Sawyer, Rosier and Phelan, 1995). This method suffers from being the most inaccurate of any available (Horn, 1999:126), however the alternative requires a series of tests that need to be administered by an HCP.
This ethnographic investigation would be open and exploratory (RPS, 1997). A system of meanings would be taken either from transcripts (Scherman and Löwhagen, 2004:4) or preferably from audio recordings as current best practice in medical market research favours working from the audio as nuances of meaning are more likely to be apparent (Kazmer & Xie, 2008).
Given the complexity of influencing compliance and the desire to use this as a measure of effective learning, structured and semi-structured in depth interviews will take place. In addition physiological improvements to lung functionality need to be measured for a sample of the participants to offer an objective indicator that a change of behaviour has occurred.
Other influences on outcomes that should be revealed in a semi-structured interview include issues of identity in relation to learning (Kirkup, 2001; and Hughes, 2007) and motivation, what Resnik (2008) describes as ‘passion based learning’.
The text from these interviews will be analysed for clusters of meaning, aiming to pick out nuanced responses, potentially from video but at least from audio recording of interviews (Kazmer & Xie, 2008), which according to Webb (2011) is preferable to working from text alone
The aim would be to reveal the experiences of those interviewed and so come to a view of ‘understandings and misunderstandings’ about their condition, the role their prescribed ‘preventer’ medication plays and the value of Qstream.
Qstream offers a variety of ways to monitor and measure activity on the platform (fig. 4) . This is how data and metadata from several hundred participants would be analysed. (Appendix 3 lists the affordances of using a Qstream private site)
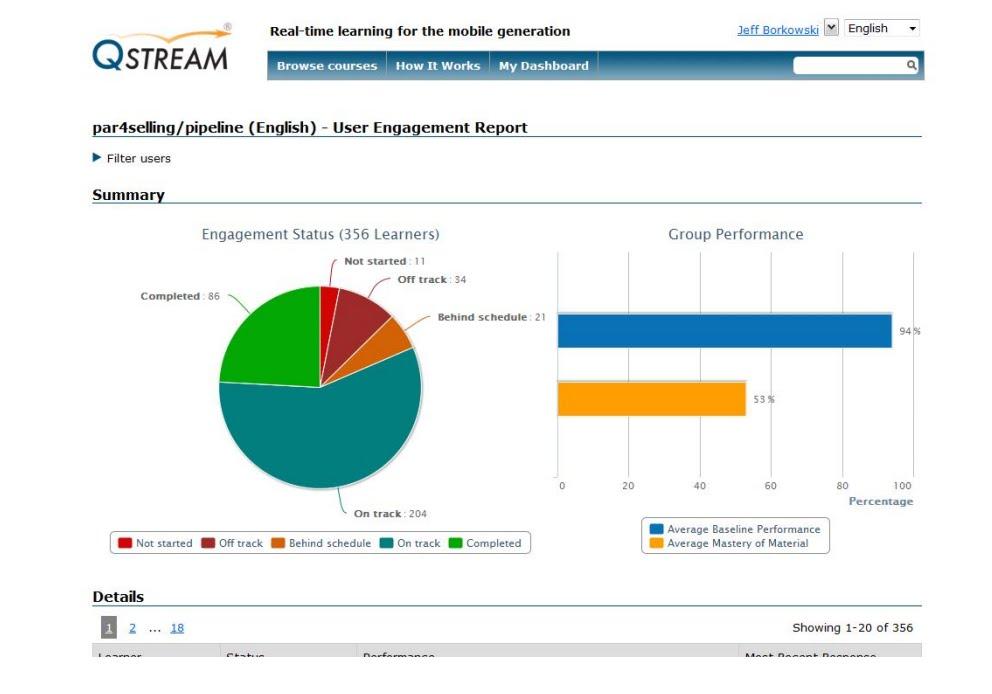
Fig. 4. Screengrab showing example of analytics available on a group of 356 learners.
TIME LINE CHART
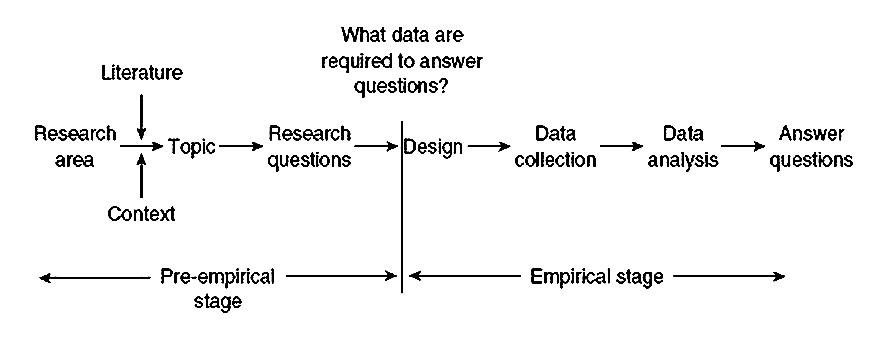
Fig. 5. Simplified model of research. Punch (2006: KL 487 )
Eligibility for interviews and physiological testing would be based on patients with the indicated symptoms though excluding patients with serious social problems and severe learning difficulties. (Franklin et al., 2006)
Aim to recruit 30+ students for in-depth interviews and <1000 for a randomized controlled trial using the Qstream platform. Confirm participants, ensure that they understand the terms and nature of the research and request that they read and agree to these and that participation is voluntary, information will be confidential and their written consent is required. Invite all or some to complete either an asthma Journal or, as they have been shown to be effective, an audio log. Patient-reported outcomes would help us understand the impact of drugs on patients’ lives and activities. “Are patients really doing better? Can they sleep through the night rather than waking up with a sense of shortness of breath?” Bohen (2013: 863)
Pre-Qstream Interviews
Run Qstream e-learning programme for 12 weeks
Post-Qstream Interviews
Analyse data and metadata generated by the Qstream platform
Write up and report findings. Follow up a year later to see if the impact of the learning is maintained over time through changing behaviours. |
Limitations
No study of a therapeutic regime can be considered fully valid without some documentation of whether the patients took their treatment. Horn (1992:127) Establishing valid data on whether people take their medication as prescribed will be a challenge.
No single method of assessment of compliance with (anti-asthma) therapy is ideal nor does any one method give a full picture of the pattern of compliance. Usually the chosen method(s) will require to be validated specifically for the particular circumstances under investigation.
An issue arises with using an Internet and mobile alert system where potentially limited or broken Internet access or paid-for Wi-Fi impinges on the student’s access to the resources. Care will be taken both over how content is scripted and produced, as well as securing a robust platform. Kerfoot and Baker (2012:13) had problems in relation to: ‘server errors’, ‘attrition’ (Kerfoot & Baker, 2012:4), ‘fatigue’ (Kerfoot et al., 2010) and technical hitches due to spam blockers (Shaw et al., 2011) as well as the challenging nature of the content. (In Vernon, 2013)
It is also reasonable to suggest that those who are noncompliant to regularly taking their prescribed medicine could also be ‘noncompliant’ to the features of Qstream – a twice or thrice weekly prompt to take a few minutes to answer some questions.
A UK license for up to 1,000 participants to use the Qstream platform is $15,000 per annum.
In research carried out by ZoRA et al. (1989). Only 1 in 17 diary sheets completed by asthmatic children (under age 14) were accurate to within 10% of the number of puffs used. Whilst the participants in this research are older, any completion of a dairy sheet will include errors and inaccuracies.
Overestimation in self-reporting is well known and probably due to a desire to please. (Cochrane, 1995. Cochrane 1998)
Failure of a therapeutic regime can only be ascribed to poor compliance if appropriate drugs are being prescribed in adequate dosage that historically has tended not to be the situation in the management of asthma. (Horn, 1992:127)
The population using the Internet is diverse. This impacts on research in relation to access and having a representative group of participants. (Eynon, 2009). The use of Qstream in a student population favours use of a mobile device for ease of response to email prompts. It is suggested that 53.7% of people in the UK will be using smartphones by 2014 with those aged 18-25 by far the largest group followed by teenagers (New Media Trend Watch, 2013) whilst it is estimated that nearly 38% will have tablets by this time. (eMarketer, 2013).
Ethics
For ethical reasons an institutional review board would be approached for approval to perform this study. (Kerfoot & Baker, 2012:2) (In Vernon, 2013)
-
A standardized form will be used to obtain informed consent from participants.
-
Well Being, confidentiality and anonymity will be stressed.
-
Rights will be clearly explained
-
The personal safety of those conducting the research will be considered.
-
Conflicts of Interest will be declared, for example, Dr Kerfoot is on the board of Qstream.
-
Unintended consequences will be considered.
-
People have to have the freedom to make mistakes in relation how they elect to adhere, or not, to the prescription drugs they are prescribed. Mental Healthcare Act.
Validity and reliability
If one hope is to correlate a physiological change with improved knowledge an array of factors need to be isolated and measured. Data from both a qualitative and a quantitative approach, the clusters of issues and ideas from analysing what is said in pre and post interviews and the activity on the Qstream platform will offer some indication of what is taking place and why.
Implications for future policies, practice and further research
1) Socio-constructed learning and connectivism
It is further hypothesized that effective compliance is most likely to be achieved where in addition to the patient, the related HCPs engage in the proposed e-learning programme. Social interaction has an important role to play in learning. (Vygotsky, 1978) Donath (2002) shows how through exchanging information a person gains recognition and that social learning of this kind provides affiliation. This suggests value in having HCPs, even family, especially parents and guardians, of younger people with asthma taking part in a Qstream learning programme and exploiting how we connect in networks (Kit Yee et al., 2011) Wang (2008:05) considers the importance in learning of both the student and instructor. HCPs would play the role of ‘intermediaries’ (Laurillard, 1993).
This not only invokes ideas of values relating to communities of practice (Lave and Wenger, 1991) but also, in our digital age, to ‘connectivism’ (Siemens, 2006; Calvani, 2009: de Waard, 2011) – where ‘nodes of readily available information’ are linked to and shared between learners. (Edudemic, 2013) The asthmatic as a learner can question their own knowledge and understanding by connecting with others, as part of a ‘community of practice’ (Lave and Wenger, 1991), from the periphery (Brown, 2002; Brown, 2007) and vicariously (Cox, 2006). Connecting with other people with asthmatics online is supported by the Asthma UK website (Asthma UK, 2013)
2) Use of narrative and creative content
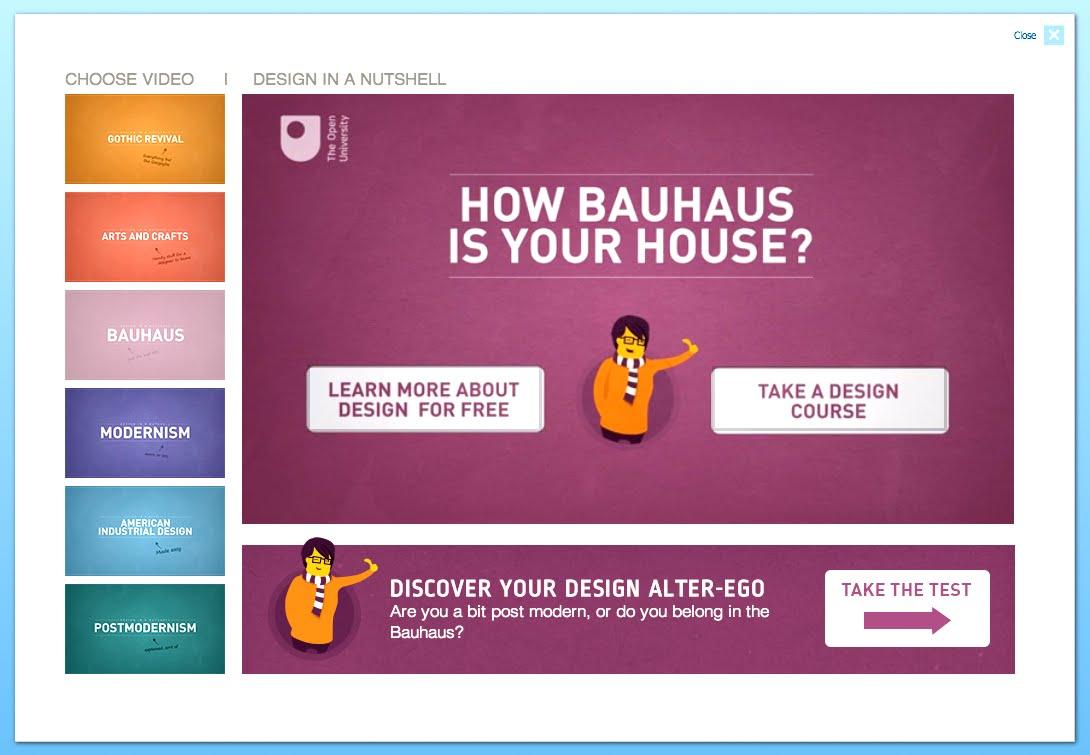
Fig. 5 Screengrab introducing a series of animated videos on design. Open Learn (2013)
The quality and style of scriptwriting using the Qstream platform will impact on effectiveness. (Laurillard, 2000 and Jewell and Hooper, 2011) understand the role of narrative in learning. Resnik and Chang (2008) talk about the need for e-learning to be self-revealing, pleasurable and fun, with a ‘low threshold and high ceiling, supporting collaboration, plugins and making it iterative’ and ‘tinkerable’. The Open University, through Open Learn, often use rich video content to engage audiences, for example with a series of short video in ‘Design in a nutshell’. (Open Learn, 2013)
3) Further personalisation of e-learning
Intelligent Web pages that can adapt themselves to a person’s linguistic and other competence are examples of more ambitious applications that we might look forward to in coming decades. (Hara et al., 2006:352)
4) Extend duration of study period
This study would initially be restricted to a single term or academic year, though it could be extended, for example, to include first year undergraduates through the 3 to 4 year duration of their undergraduate studies. Ostojic et al., (2005) carried out a 4-month trial, whilst trials run by Kerfoot (2008-2012) have run for as long as 45 weeks.
5) Include other chronic illnesses:
Allergic rhinitis is comorbid with asthma (Bousquet at al., 2013) warranting its inclusion in future research alongside studies on asthma. Other chronic illnesses that may benefit from Qstream’s use by patients includes diabetes, epilepsy, Parkinson’s and Alzheimer’s.
6) Consider ‘Big Data’, Web 2.0, Pedagogy 2.0
There is the potential of automatic real-time data gathering relating to inhaler use with a microchip and the use of wearable technology even an ingestible smart pill (Engineer Online 2012; Arnold, 2013) in medicine. Supported by enhanced patient knowledge of their illness. Armed with this data, analysed automatically, and read by the patient or an HCP, the drug regimen and response to it is closely monitored. Such patient analytics are akin to student performance analytics (Koller, 2012) providing HCPS and educators with the potential for gathering and analysing data and metadata from hundreds of thousands of participants.
Conclusion
The opportunity exists to develop an e-learning programme that change lives – that improves the health of those with moderate to persistent asthma. Research suggests that greater knowledge and understanding of a chronic medical condition and personal medical and lifestyle responses and self-management improves compliance. However, the way the illness presents are complex, the triggers and symptoms vary greatly. The approach suggested here also offers the chance to establish if learning brings about a change in behaviour that can be measured in a physiological response – improved lung function and the role an e-learning platform can play. In due course, if a reasonable percentage of the 300+ million asthmatics who are online engage with an e-learning programme such as this significant insights and improvements to health can be made.
REFERENCES
Adams, S., Pill, R., Jones, A. (1997) Medication, chronic illness and identity: the perspective of people with asthma. Soc Sci Med 1997; 45:189-201
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (Revised 5th ed.). Washington, DC: Author.
Arnold, M (2013), ‘A VIEW TO A PILL. (cover story)’, Medical Marketing & Media, 48, 6, pp. 26-30, Business Source Complete, EBSCOhost, viewed 26 June 2013.
Asthma UK (2013) Asthma facts and FAQs. http://www.asthma.org.uk/asthma-facts-and-statistics (Accessed 23rd June 2013)
Bohen, S (2010) Sean Bohen, senior vice president of early development at Genentech (in Smith, B 2010. The Future of Pharma)
Bousquet, J, Khaltaev, N, Cruz, A, Denburg, J, Fokkens, W, Togias, A, Zuberbier, T, Baena-Cagnani, C, Canonica, G, Van Weel, C, Agache, I, Aït-Khaled, N, Bachert, C, Blaiss, M, Bonini, S, Boulet, L, Bousquet, P, Camargos, P, Carlsen, K, & Chen, Y 2008, ‘Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN’, Allergy, 63, pp. 8-160, Academic Search Complete, EBSCOhost, (Accessed 19 June 2013).
Brown, J.S. (2002) The Social Life of Information
Brown, J.S. (2007) October 2007 webcast:http://stadium.open.ac.uk/stadia/preview.php?whichevent=1063&s=31
Calvani, A. (2009). Connectivism: new paradigm or fascinating pot-pourri?. Journal of E-learning and Knowledge Society, 4(1).
Cerveri, I ; Locatelli, F ; Zoia, MC ; Corsico, A ; Accordini , S ; de Marco, R. (1999) International variations in asthma treatment compliance – The results of the European Community Respiratory Health Survey (ECRHS) EUROPEAN RESPIRATORY JOURNAL Volume: 14 Issue: 2 Pages: 288-294 DOI: 10.1034/j.1399-3003.1999.14b09.x Published: AUG 1999 (Accessed 21st June 2013)
Cox, R. (2006) Vicarious Learning and Case-based Teaching of Clinical Reasoning Skills (2004–2006) [online], http://www.tlrp.org/proj/phase111/cox.htm (Accessed 25 June 2013).
de Waard, I. (2011). Explore a new learning frontier: MOOCs. Retrieved from Learning Solutions Magazine website: http://bit. ly/mSi4q
Dukes, DE 2001, ‘What You Should Know about Direct-to-Consumer Advertising of Prescription Drugs’, Defense Counsel Journal, 68, 1, p. 36, Business Source Complete, EBSCOhost, (Accessed 24 June 2013).
Ebbinghaus, M (1913) Memory: A contribution to experimental psychology. (translated by H. A. Ruger and Clara E. Bussenius) 1913, (New York: Teachers College Press),
Edudemic (2013) A simple guide to 4 complex learning theories. http://www.edudemic.com/2012/12/a-simple-guide-to-4-complex-learning-theories/ (Accessed 23 June 2013)
E-Learning Council (2013) Overcoming the Ebbinhause Curve – How we soon forget. http://www.elearningcouncil.com/content/overcoming-ebbinghaus-curve-how-soon-we-forget. (Accessed 23 June 2012)
E-Marketer (2013) UK Tablet use sees robust growth. http://www.emarketer.com/Article/UK-Tablet-Use-Sees-Robust-Growth/1009857 (Accessed 23 June 2013)
Engineer Online (2012) ‘Smart pill containing microchip tracks adherence to medication’ 2012, Engineer (Online Edition), p. 12, Business Source Complete, EBSCOhost, (Accessed 26 June 2013).
Hammersley, M. (1992) What’s Wrong with Ethnography. London: Routledge.
Hayes, R.B., Taylor, D.W., Sacket, D.L. (1979) Compliance in health care. Baltimore: John Hopkins University Press.
Horne, R., & Weinman, J. (2002). Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychology and Health, 17, 17–32. doi:10.1080/08870440290001502
Hughes, G. (2007) ‘Diversity, identity and belonging in e-learning communities: some theories and paradoxes’, Teaching in Higher Education, vol. 12, no. 5, pp. 709-720.
(access 24 June 2013)
Inkpen, K.M. (2000) Designing Handheld Technologies for Kids, Personal Technologies, 3(1-2): 81-9.
Kerfoot, B.P., Armstrong E.G., O’Sullivan P.N. (2008) Interactive spaced education to teach the physical examination: a randomized controlled trial. J Gen Intern Med 2008;23:973–978.
Kerfoot, B.P. (2009) Learning benefits of on-line spaced education persist for 2 years. J Urol 2009;181:2671–2673.
Kerfoot, B.P, Kearney MC, Connelly D, Ritchey ML. (2009) Interactive spaced education to assess and improve knowledge of clinical practice guidelines: a randomized controlled trial. Ann Surg 2009;249:744–749.
Kerfoot, B.P, Lawler EV, Sokolovskaya G, et al. (2010) Durable improvements in prostate cancer screening from online spaced education a randomized controlled trial. Am J Prev Med 2010;39:472– 478.
Kerfoot, B.P., Baker, H., (2012) An Online Spaced-Education Game for Global Continuing Medical Education: A Randomized Trial. Annals of Surgery Volume 256, Number 1, July 2012. pp.1227-1232 www.annalsofsurgery.com
Kerfoot, B.P., Baker, H., Pangaro, L., Agarwal, K., Taffet,G., Mechaber, A.J., Armstrong, E.G. (2012) An Online Spaced-Education Game to Teach and Assess Medical Students: A Multi-Institutional Prospective Trial. Technology and Learning. Academic Medicine, Vol. 87, No. 10 / October 2012 pp. 1443 – 1449
Kirkup, G. (2001) Getting our hands on IT. Gendered inequality in access to ICTs. Conference paper at Gender and Virtual Learning, Hagen, Germany.
Kit Yee, A, Moon, G, Robertson, T, DiCarlo, L, Epstein, M, Weis, S, Reves, R, & Engel, G (2011), ‘Early Clinical Experience With Networked System for Promoting Patient Self-Management’, American Journal Of Managed Care, 17, 7, pp. e277-e287, Academic Search Complete, EBSCOhost, (viewed 19 June 2013).
Koller, D (2012) What we’re learning from online education http://www.youtube.com/watch?feature=player_embedded&v=U6FvJ6jMGHU (Accessed 24 June 2013)
Laurillard, D. (1993). Rethinking university teaching: A framework for the effective use of educational technology.
Lave, J, and Wenger, E. (1991) Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge University Press.
New Media Trend Watch (2013) http://www.newmediatrendwatch.com/markets-by-country/18-uk/154-mobile-devices (Accessed 23 June 2013)
NHS Choices. Health A-Z. Asthma. http://www.nhs.uk/conditions/asthma/Pages/Introduction.aspx (Accessed 23rd June 2013)
Offer, D, Ostrov, E., Howard, K.I. (1977) The Offer Self-Image Questionnaire for Adolescents. A manual, revised. University of Chicago, Illinois.
Open Learn (2013) Design in a nutshell. http://www.open.edu/openlearn/science-maths-technology/engineering-and-technology/design-and-innovation/design/design-nutshell (Accessed 26 June 2013)
Picard, R, Papert, S, Bender, W, Blumberg, B, Breazeal, C, Cavallo, D, Machover, T, Resnick, M, Roy, D, & Strohecker, C (2004) ‘Affective learning – a manifesto’, Bt Technology Journal, 22, 4, pp. 253-269, Science Citation Index, EBSCOhost, (viewed 24 June 2013).
Perlin, K. and Fox, D. (1993) Pad: An Alternative Approach to the Computer Interface, Proceedings of SIGGRAPH ’93:20th Annual Conference on Computer Graphics and Interactive Techniques, 2-6 August 1993, Anaheim, California, USA, 93:57-64.
Petrie K.J., Perry, K., Broadbend, E., Wienman, J (2012) A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication’.
Punch, K.F. (2006) 2nd Edition. Developing Effective Research Proposals.
Resnik, M and Chang, A (2008) Tinkering Together: enabling synchronous creativity and distributed collaboration for kids, MAS 712 Technologies for creative learning.
Royal Pharmaceutical Society (RPS) of Great Britain. (1997) From compliance to concordance: achieving shared goals in medicine taking. London: Royal Pharmaceutical Society of Great Britain
Sawyer, S., Rosier, M. J., & Phelan, P. (1995). The self-image of adolescents with cystic fibrosis. Journal of Adolescent Health, 16(3), 204–208.
Sharples, M., Corlett, D. and Westmancot, O. (2002) The design and implementation of a mobile resource, Personal and Ubiquitous Computing, 6: 220-34.
Soloway, E, Norris, C, Blumenfeld, P, Fishman, B, Krajcik, J, & Marx, R 2001, ‘Handheld Devices are Ready-at-Hand’, Communications Of The ACM, 44, 6, pp. 15-20, Business Source Complete, EBSCOhost, (Accessed 24 June 2013).
Stenhouse, L. (1981) ‘What counts as research?’, British Journal of Educational Studies, vol. 29, no. 2, pp. 103
Scherman, M, & Lawhagen, O (2004), ‘Drug compliance and identity: reasons for non-compliance : experiences of medication from persons with asthma/allergy’, Patient Education & Counseling, 54, 1, pp. 3-9, CINAHL, EBSCOhost, (viewed 12 March 2013).
Siemens, G. (2006). Connectivism: Learning theory or pastime of the self-amused.Retrieved February, 2, 2008.
The Student Room (2013) http://www.thestudentroom.co.uk/ (Accessed 26 June 2013)
Vernon, J.F. (2011) Practice-based research in e-learning (H809). Tutor Marked Assignment 1 (TMA01)
Vernon, J.F., and Kerfoot, B.P. (2013) Skype conversation on the use of e-learning in healthcare in relation to people with chronic illnesses. Considered H809 TMA01. (Unrecorded)
Wang, M., Shen, R., Novak D. and Pan, X. (2008) ‘The impact of mobile learning on students’ learning behaviours and performance: report from a large blended classroom’, British Journal of Educational Technology.
Webb, S (2011) ‘Attacks on asthma’, Nature Biotechnology, 29, 10, pp. 860-863, Academic Search Complete, EBSCOhost, (viewed 12 June 2013).
Wokasch, M. (2010) Pharmaplasia. Wokasch Consulting LLC.
APPENDIX ONE
How to define asthma
MODERATE PERSISTENT – IN THE RESEARCH GROUP (aboutasthma.com)
Your asthma severity is classified as moderate persistent asthma when:
With moderate persistent asthma, you will need daily asthma medication with anti-inflammatory properties, as well as a second medication. You are able to gain control of your asthma with two medications, what we call the ‘blue one’ and the ‘brown one’. The brown one, the inhaled steroid, you take a couple of puffs in the morning and a couple at night. The blue one, the reliever, or what in North America they call the ‘rescue’ inhaler, you take as required Source: National Heart, Lung, and Blood Institute. Accessed: May 20, 2010. Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma |
APPENDIX 2
|
% =/-5% too ill to attend ‘profound’ SOTON 17000 undergraduates First years 5,000 – 5,500 |
Total Soton 9.5% |
Total Soton 11.5% |
First Years 9.5% |
First Years 11.5% |
Across4 UK universities |
|
Approx: students with asthma in the undergraduate population |
1,615 |
1,955 |
475 |
575 |
64,500 |
|
Describing themselves as: 41% very mild |
662 |
801 |
195 |
234 |
26,445 |
|
27% mild |
436 |
528 |
128 |
155 |
17,415 |
|
19% moderate |
307 |
371 |
90 |
109 |
12,255 |
|
11% severe (Wales et al., 2011) |
178 |
215 |
52 |
63 |
7,095 |
|
Moderate to severe likely to be: |
485 |
586 |
142 |
172 |
19,350 |
|
48% think they are at risk (Asthma UK) |
232 |
263 |
68 |
82 |
3,405 |
|
53.7% smartphones by 2014
|
125 |
141 |
37 |
44 |
1,829 |
|
less 4% self exclude from digital devices |
120 |
135 |
36 |
42 |
1,756 |
University of Southampton
Of an undergraduate population at the university of Southampton of 17,000 UK asthma statistics (Asthma UK, 2013) would suggest that between 1 in 10 and 1 in 12 are asthmatic (in a school population 1 in 12 has asthma, while there are 1 in 10 in the general population). Of these 5% have severe asthma and are unlikely to be attending university. This would suggest that between 9.5% and 11.5% as asthmatic. So between 1,615 and 1,955 asthmatic, of whom 662 to 801 likely to say that they are very mild and from 436 to 528 mild so have no medication, or a reliever at most (if they’re right). Between 307 and 371 moderate and 178 to 215 severe – so likely to be on a reliever at least at one end of the spectrum and a preventer too towards the more persistent or severe levels. i.e from 485 to 586. Of these 232 to 263 are likely to think they are ‘at risk’ (Asthma UK). Horn (1992) suggests that patients who admit to poor compliance may be more amenable to compliance modifying strategies; EU funded research into asthma has shown a significant willingness of those with this troublesome disease to take part in research (Cerveri et al., 2013) Whilst use of a smartphone does not define a person as digitally literate a self-reporting interview will isolate those who are … which might be, given use of e-learning in higher education, most of this group. A further reduction is given to exclude some who will not use these devices.
Potentially conducted across four universities:
- University of Southampton. 17,000 students.
- City University, Finsbury, London. 17,000 students. Urban
- University of Cumbria in Lancaster and Newton Rigg, Penrith. 10,500 students. Rural
- University of Oxford. 20,000 students.
APPENDIX THREE
Benefits of a private site using Qstream
|
User admin |
Batch invite |
|
Batch enroll |
|
|
History – invite, enroll |
|
|
Delete |
|
|
Email issue mgmt |
|
|
User registration report |
|
|
Access to learner email addresses |
|
Reporting & analytics |
User tagging |
|
Management roles & reporting |
|
|
Management summary engagement emails (weekly) |
|
|
Engagement summary |
|
|
Engagement detail & export |
|
|
Learner performance summary |
|
|
Learner performance detail & export |
|
|
Snapshot analytics |
|
|
Trend analytics |
|
|
Question performance report |
|
|
Question performance answer matrix |
|
|
Question performance analytics |
|
Site admin |
Monitor site activity |
|
Monitor comment activity for site |
|
|
Site branding (logo, tagline, home page, Dashboard, URL) |
|
|
Site localization (site branding translations) |
|
|
Email branding (sender name, organization logo) |
|
|
Private site publishing privileges |
|
Course admin |
Manage comment activity for course |
|
Shut down courses |
|
|
Basic course branding (course logo, course title) |
|
|
Adv course branding (sender name, organization logo) |
|
|
Private course catalog |
|
|
Public course catalog listing |
|
|
Private, closed courses |
|
|
Open enrollment courses |
|
|
Control course ‘operations’ (spacing, locked/unlocked) |
|
|
Completion management (%, certificate, messaging) |
|
|
Assign authors, co-authors |
|
|
Assign moderators |
|
Learner experience |
Customized leaderboard gaming (email display, online display, invid, team, monthly, rollilng) |
|
Localization |
|
|
Mobile |
Native app with notifications |
|
Mobile interface |
|
|
Course authoring |
Course catalog description/listing |
|
4 question types (MC, MCA, T/F, FIB) |
|
|
Preview/validation of questions |
|
|
Security |
Auto login |
|
Data security |
|
Social & collaboration |
Assign course moderator |
|
Learners can post private or public comments |
|
|
Comment management tools |
Selecting a topic and title. H818 Activity 3.1.

Fig.1. Listening to a memorable and evocative ‘visitor audio tour’ on Alcatraz. Away from the bustle of people, by a nature reserve for nesting gannets.
1) Theme and Format. Presentation of a multimedia model, QStream, for use before, during and after a trip that might be to a museum, historic property or battlefield.
2) With the centenary of the First World War upon us I would like to find ways to enhance the visitor experience, perhaps for those with a GCSE or A’Level, or an undergraduate interest rather than for the general public. Ideally there would be options to select a level of interest and previous understanding.
3) For this audience Secondary or Tertiary audiences will be of most interest. Perhaps even promoting an MA course for graduate Historians?
4) I have had an interest in QStream for a couple of years and developed a proposal for its use with patients with chronic illness. This is an alternative, though equally valid use for the platform. My only variation on this would be to include an audio component, and/or to track visitors so that content might be tailor to and for them.
5) How an App that spaces learning over a period of weeks and months can support the experience of visiting a museum, historic property or battlefield.
How an App is able to create a personalised experience for a visitor to a museum, historic property or battlefield that enhances the learning experience without distracting from the artefacts or the place itself, in other words, in compliments and augments the experience created by the visitor on their trip.
6) Already familiar with QStream (aka Spaced-Ed) I checked on latest papers and developments. I searched ‘museum’, ‘augmented’ and ‘elearning’ and from a selection of around 12 papers have thus far read, in depth, two of these as well as a couple of commercial conference presentations of a museum platform. Based on this the idea is shifting towards headphones tracked in a space feeding a bespoke sound landscape and commentary based on where a person is and their observed and apparent behaviour. One platform avoided the need for any input by the user, though for my purposes GCSE (Key Stage X), A’leve (Key Stage Y) or Undergraduate, even Graduate is considered necessary so that you compliment the person’s necessary learning experience.
7) My literature research approach can always be refined, having completed H809 Research-based practices in online learning I feel competent to conduct a thorough search.
8) One glitch was to in error delete a folder in RefWorks rather than create a bibliography. There was no back button to undo. I make look at purchasing a commercial referencing tool such as EndNote. Having always felt that online learning was a process I felt the need to have a subject specialism too, for this reason I am taking a Masters degree in British First World War studies with the University of Birmingham. This is a very different experience. A monthly day of lectures/tutorial, a reading list with books to find from a regional university library, and an online platform that makes the OU VLE look like Whisley to Bham’s assorted allotments under the railway bridge! But you do get to meet fellow students and librarians.
9) Audio, without visuals, feelslike harking back to audioguides of the 1980s and 1990s, yet today, with GPS and other sophisticated tracking devices a visitor experience can be situated, to the spot, personalised to the individual, and still be evocative through ‘painting pictures’ in the mind without distracting from artefacts museum curators have so carefully chosen. A recent experience visiting Alcatraz, for all its Disneyfication and complimentary wildlife sanctuary cum Native American protest camp, included what I would describe as a BBC Radio 4 docudrama that was intelligent, moving an engaging – a blend of officer, prisoner and officer family oral memoir and soundscape. However, it did rely on the visitor being in the right spot when the audio was played so that very quickly, taking my own route around the island, I found the content in my head at odds, in an interesting way, with what I was looking at: gannets nesting on an old basketball yard (making it akin to a visit to the Farne Islands or the Bass Rock, also an old prison) while in the distance multimillion dollar multi-hull yachts raced the America’s cup.
On Reflection
The experience of Alcatraz would be extended if I had this audio-tour still to listen to repeatedly, to read as a transcript and then to find links for my own research. Having circumvented the regular tour I nearly found myself embarking with the headphones still plugged in … I’m like the characters in ‘Jurassic Park’, I soon tire of someone else’s plot and create my own journey. It gave new meaning to the ‘birdman’ of Alcatraz, for example. And I can see why Clint Eastwood would never have made it to land … you’d be washed out into the Pacific.
Kiss the frog
Fig.1. ELearning Network team exercise
Throughout my career I have relished the company of like-minds that comes from being part of a ‘trade association’. Since I was a teenager I was part of the IVCA – the communications industry and the extensive use of video in training and communications.
Over the last decade, with the digital takeover and the demise of video in favour of faster, personalised delivery mechanism and smart learning online new associations have emerged. Personally, a Master of Arts in Open and Distance Education (MA ODE) has convinced me that video is a blunt, even bland and potentially forgettable and disengaging response to a learning need – well written text can be read at a pace set by the participant.
I joined the ELearning Network doing a bit online and following various stories. Last Friday I joined 30 or so for a day long series of talks. I was impressed. It worked.
Over the course of five hours there were five presenters – the format was engagement rather than lecture.
It gave me the perspective of the industry I wanted as I contemplate taking my interest in an academic approach to the next step – PhD research.
Where is the ‘smart e-learning’ and what can I isolate into a piece of original research that warrants three years of research and a 100,000 thesis?
I gained insights on:
- Composing questions
- The role of games and gamification
- Tools
- Design for social interaction
- Designing interaction: games, social, tutorial …
In the process our table invented a game called ‘Kiss the Frog’ where participants have to battle against the odds and each other to ‘kiss the frog’ – so that they too can become a frog and live happily ever after and a game to explain genetics in relation to colour-blindness.
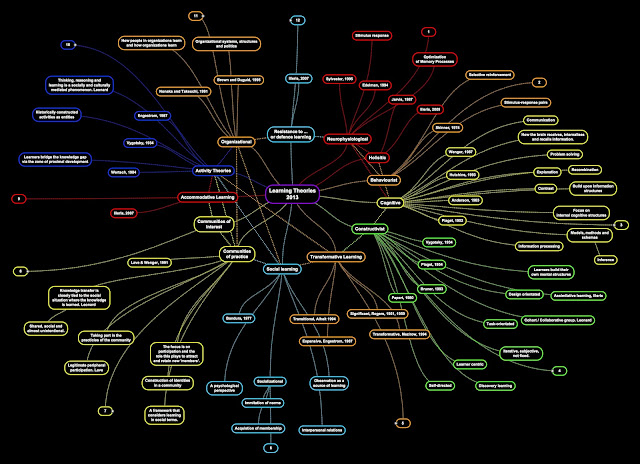
13 E-learning theories
|
Associative/ Behaviourist approaches
|
Design principles
|
|
Looking for observable behaviour
|
Explicitly mentioning course outcomes
|
|
Behavioural objectives
|
Ability to test achievement of learning outcomes
|
|
Instructional Systems Design (ISD)
|
Decomposing learning into small chunks
|
|
Routines of organised activity
|
|
|
Learning hierarchies (controversial!)
|
Sequencing learning materials with increasing complexity
|
|
Giving direct feedback on learning
|
|
|
Individualized learning trajectories
|
|
|
Cognitive psychology (constructivism)
|
|
|
Types of memory (sensory – short term – long term)
|
Maximize sensations: strategic screen layout
|
|
Research on memory, perception, reasoning, concept formation.
|
Maximize sensations: well-paced information
|
|
Learning is active
|
Maximize sensations: highlighting main elements
|
|
Learning is individual (knowledge construction)
|
Relate difficulty level to cognitive level of learner: providing links to easier and more advanced resources
|
|
Use of comparative advance organizers
|
|
|
Use of conceptual models
|
|
|
Importance of prior knowledge structures
|
Pre-instructional & prerequisite questions
|
|
Experimentation toward discovery of broad principles
|
|
|
Promote deep processing
|
Use of information maps zooming in/ out
|
|
Cognitive Apprenticeship (Brown et al, 1989)
|
Interactive environments for construction of understanding
|
|
Metacognition (reflection, self-regulation)
|
Relate to real-life (apply, analyse, synthesize)
|
|
Learning styles (controversial!)
|
Address various learning styles
|
|
Cognitive styles
|
Let students prepare a journal
|
|
Dual coding theory
|
Use both visual information and text
|
|
Motivate learners (ARCS model)
|
Use techniques to catch attention, explain relevance, build confidence and increase satisfaction
|
|
Situated learning (constructivism)
|
|
|
Personal knowledge construction
|
Personal meaning to learning
|
|
Situated learning: motivation
|
Relate to real life (relevance)
|
|
Holistic/ Systemic approaches
|
Conduct research on internet
|
|
Build confidence with learners
|
|
|
Identity development
|
Use of first-hand information (not filtered by instructor)
|
|
Communities of Practice (Lave & Wenger)
|
Collaborative activities
|
|
Zone of Proximal Development (Vygotsky)
|
Fostering the growth of learning communities
|
|
Learning as act of participation
|
Legitimate (peripheral) practice, apprenticeships
|
|
Lifelong learning
|
Authentic learning and assessment tasks
|
|
Connectivism
|
|
|
Information explosion
|
Digital literacies
|
|
Learning in network environment
|
Keep up-to-date in field
|
|
Knowledge base
|
Multi-channel learning
|
|
Distributed learning
|
Build diversity, openness in learning (different opinions), autonomy
|
|
Personal Learning Environment
|
self-directed learning, just-in-time |
Constructivism – Jonassen et al 1999
Social Constructions – Vygotsky 1986
Activity Theory – Engeström et al 1999
Experiational Learning – Kolb 1984
Instructional Design – Gagné et al 2004
Networked and collaborative work – McConnell 2000
Learning Design Jochems et al 2004
Primary: presenting information
Secondary: active learning and feedback
Tertiary: dialogue and new learning.
Related articles
- Module 3 – Learning and Technology Theories Reflection (natalieedit202.wordpress.com)
- Learning Theory (downes.ca)
- Learning Theory – What are the established learning theories? (miracletrain2013.wordpress.com)
- Learning Theories and Technology (daniellegroten.wordpress.com)
- Connectivism: A Learning Theory for the Digital Age (gamedynamics.wordpress.com)
- Social Constructivism (s4323697.wordpress.com)
Methodological Innovation
From the Oxford Internet Institute
Methodological innovation is vital given the changing nature of the Internet and advances in ICTs which both necessitate and facilitate the development of new techniques.
OII researchers are developing methodologies such as:
- big data approaches;
- the embedding of ICT s for real time observation of social phenomenon;
- webmetric techniques for observing the underlying structure of the web presence of social institutions;
- artificial intelligence design;
- experimental research;
- on-line action research;
- content analysis;
- investigation of virtual environments;
- and online survey research.
The five current research foci examine the role of the Internet and other ICTs in:
- government and democracy: where ICT s offer significant opportunities for restructuring practices and institutions, for example in the management and delivery of government services and the functioning of governance processes
- research and learning: focusing on the use and impact of ICTs within academic and research communities and the social and institutional contexts in which this takes place
- everyday life and work: covering the role of the Internet and other ICTs in personal interactions in the household, the arts, and entertainment, and the needs of individuals and the wider community in work, social relationships, leisure, and activities in other arenas that bring society online
- shaping the Internet: how rapidly developing ICTs are liberated or constrained, including how the Internet itself is governed.
- network economy: how ICTs reshape business models, markets and economic development.
Unscrambling the presumptions of research in e-learning educational practice
Activity Theory (AT) according to various authors …. , supposes a quest to solve a problem, an ‘activity theorist’ looking at certain kinds of research, understanding activity system as being driven by outcomes, would therefore annotated the six nodes of the AT pyramid with this in mind.
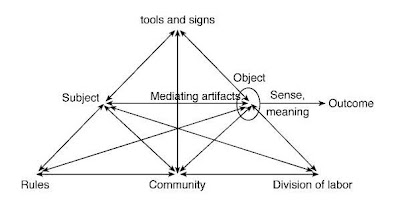
Fig. 1. Activity Theory (Engeström, 2008)
In contrast, considering the same subject of research, a sociologist would be inclined to look for power structures.
In turn how might a management consultant, or psychologist approach this? And in relation to H809 and the MAODE, how differently would someone educated in each of the following theories approach the same subject matter: behaviorism, cognitivism, constructivism and connectedness?
The suggestion that the theory behind a piece of research or OER from H809 TMA02 predisposes a specific research response is like having an undefined medical problem. In turn each specialist offers a view based on the narrow perspective of their specialism.
By way of example, with sinus/earache like symptoms from which I have always ‘suffered’ I in turn visit a neurologist, immunologist and dentist. I discover from each in turn that I must be depressed/stressed, have an allergic response to something, need a tooth filled/crowned. In turns out that I have a pronounced response to house dust mite and due to physical damage to a channel in one part of the maxillary sinus it doesn’t drain so the slightest infection, a mild cold, will cause inflammation and pain. The response that works is primarily preventative with self-medication of prescription pain relief at a dosage that works – co-codomol and occasional antibiotics. (The above over a 33 year period of investigations that included several other excitable consultants who each in turn gleefully hoped that I might have a very rare condition X or Y that they would investigate).
Just as medical specialists are inclined to come at a situation with too narrow a perspective, so too can we when wishing to study, in a learning situation, what is going on … in there (the brains of each student) and externally, the context and situation of the ‘learning’ that they are doing (or having done to them).
Reference
Conole, G., and Oliver, M. (eds.) (2008) Contemporary perspective in e-learning research. Themes, Methods and Impacts on Practice.
Engestrom, Y (2008) From Teams to Knots
