Home » E-Learning » MA in Open & Distance Education » H809: Practice-based research in educational technology
Category Archives: H809: Practice-based research in educational technology
What is learning?
 |
| From E-Learning V |
Fig.1. Learning that is connected, socialised and shared
Does learning happen within the head of an individual, or is it mediated, situated and distributed?
Learning as an artefact is the potential informed or insightful response in an individual’s brain. Learning as a process includes the mechanisms of the brain and everything that person perceives around them – which must indirectly include everything they’ve laid down in their memory and how the subconscious responds to any of it.
What does a test or exam measure?
A test or exam can only be judged by how it is constructed and where and how it fits into a period of study – is the test part of the learning process or an assessment? Are the questions open or closed? Are their significant time constraints or not? So they should test what they were designed to test.
A response to any challenge: it takes time, experience, risk and a sense of what you are capable of

Fig.1 The only time I ever got down this precipitous drop in one go, falling the fall line, was as a fit and by then experienced skier. Plagne-Bellecote, France.
It took eight years, a badly smashed leg, both thumbs and a rib. It is thirty years since I have been in the flat we used then – this is the view from the window. I have no intentions of getting any closer than this. Instead I will join the Ski Club of Great Britain Guide and in so doing learn from others and remain in one, unbroken piece.
My H818: The Networked Practitioner
Though I completed the Master of Arts: Open and Distance Education (MAODE) last year I didn’t feel like a ‘master’ – further modules as continual professional development have realised this: H809 for research and H818 for applying and sharing in an open and ‘directed’ way. My background is a producer in corporate L&D so the aim has been to support the shift from linear to interactive, to connected and open learning founded on applied knowledge of a number of learning theories.
H818 pulled together or touched on a number of personal interests:
- Can creativity be taught or managed online?
- What are the parameters, pitfalls and potential of open learning?
- Recognition not just of an interface between online and ‘offline’ learning, but the blended mix where lessons from either world can inform the other.
There’s a difference between open (small ‘o’) and Open (large O): the latter, as I have done over 14 years posting content, is akin to ‘exposure’ – putting it all out there; whereas the Open movement to be effective, ironically, requires parameters and goals. From H818 the need to, reasons to and how to ‘ask’ became apparent.
The outcome of H818 is the Quick Response code in a Poppy to support open and connected learning about the First World War. As a creative exercise despite being unable to single out a ‘partner’ the working process has been akin to that in advertising where the creative team is a copywriter and a visualiser, with one if these or both likely to have programming skills – or the creative team becomes three. Openstudio online is like the studio I worked in at the School of Communications Arts where I was a student and now mentor.
The ask component has two parts to it:
I post then share blog posts on the QR Code idea via WordPress and a number of platforms: LinkedIn, Google+, Twitter, Facebook, Pinterest and Stumbleupon. This at best makes serendipity a possibility but is small ‘o’ – though the connections directly from this include BBC TV, BBC Radio 4, the national trust, King’s College London and a couple of people with direct, personal connection to the content I have posted – they recognise a face from a 1918 postcard.
The second part is, still early days, putting the idea to individuals and groups directly and asking questions that I take care to recognise where they are forthcoming. Using the above social platforms the request is directed at an individual, or to a specific specialist group. The ‘use of QR codes’ in education has uncovered far greater use and interest than the current papers suggest. Direct questions have gone to niche interest groups such that ‘talks’ on the use of QR codes in this way will be given to schools and to regional history associations. Not all that I approach have responded – this kind of ‘ask’ is a kind of selling or PR. It isn’t simply connectedness, it is networking too that expects a professional offering and response. ‘Consultancy’ is one thing, but the production side of it – seeing content successfully briefed in, financed, designed, scripted and delivered is my aim and so with tentative steps ‘Mindbursts’ is coming to fruition and will build on some 15 years of creating learning content in the corporate sector.
The second outcome of H818 is to try and continue and build on the relationships that were developed. In LinkedIn two groups have been set up: ‘The online masters’ and ‘MAODE’ – early days, but experience from the Open University Business School shows how from tiny beginnings great things can grew. The challenge in the early days will be to keep the kindle alight so that there is just enough ‘vibrancy’ to make it a worthwhile place for current and future members. Similarly, a blog where all members have ‘editor’ rights has been set up.
Returning to the idea of big ‘O’ and little ‘o’ it strikes me that my little ‘o’ behaviour is akin to being loudly in a crowd while big ‘O’ requires directed engagement and responsiveness. Which has me wondering that a journalist writing for a paper with its parameters and audience is more open than hiding behind the obfuscation of the blog. Which in turn, as has occurred throughout H818 has seen me completing a huge loop into an online world of the possible to the offline world of the actual and realising that quicker than I imagined learning is increasingly blended whether you put an ‘e’ or an ‘o’ or an ‘m’ in front of it.
My MAODE
My Masters in Open and Distance Education (MAODE) with the Open University (OU)
H807: Innovations in eLearning – Learning outcomes
H800: Technology-enhanced learning: practices and debates
B822: Creativity, Innovation and Change
H808: The e-learning professional
H810: Accessible online learning: supporting disabled students
This completes the Masters in Open and Distance Education (MAODE)
Taken in addition as continual professional development
H809 Practice-based research in educational technology
H818: The Networked Practitioner
An ethnographic look at how people behave online in virtual worlds compare to who they are in the real world

I went to Oxford to attend a lunchtime lecture hosted by the Oxford Internet Institute and the Institute of Social and Cultural Anthropology – anyone can attend.
I stumbled upon the talk, I asked, they said come along.
Everyone else was an OII doctoral research student.
My interest was in the explorative method, a reminder of how anthropologists study ‘in the field’ and as much as anything else its an opportunity to talk to and meet people with similar interests.
Three years online and if I continue it will be lectures and face to face – or blended.
I gave myself three hours to get there – just as well as there were accidents on both the M23 and M25. Coming back … more accidents, a 40 mile tailback. I pulled into a service station for 90 minutes
The M25 was designed as a river, it’s turned into a glacier.
Dr William Kelly is Research Associate at the School of Anthropology and Museum Studies and Professor at the School of Global Studies, Tama University (Tokyo). He gave a talk on what he is learning about Japanese Virtual Worlds by talking to the creators of specialist niche environments for Japanese people.
QUESTIONS
How to study expressions of culture in a virtual space.
THEMES
Started to think about questions on:
- expression of identity/self–hood –self–presentation,
- fashion/adornment, body type.
- concepts of utilization of space, as building things – how after work group socializing, what some of patterns do they replicate.
- patterns of social interaction
Culturally specific venues and services – Japan for Japanese, Non–Japanese for Japan, and enthusiasts.
ISSUES
Identifying field sites
Handling offline and online – Japanese write nothing of their offline world.
Ethical
Protection of privacy and permissions.
METHODOLOGY
Company visits and interviews
Contacting producers, visit Tokyo
What is their business in Second Life.
How do they contact and interact with consumers
FINDINGS
People who are very well socialised in the online world, and well socialised in the offline world, which is where my interest took me. (Anthropologist). i.e field study.
Are people being themselves or schizophrenic online … and where is the development of the person occurring? Between the two? WK thinks between the two. Many typing v fast, not speaking. Like John Travolta in Saturday Night Fever? Are deceptions successfully played out in VW.
A given in Second Life that everyone is an avatar. Everything is a pseudonym. e.g. an architect in real life who is extremely active and fast in Second Life too. Some have a strong professional engagement, for others it is clearly escape from hard lives.
Two Virtual Worlds (VW) were studied and two specialist creators of content for these VWs. The worlds were the Japanese world within Second Life and a VW recreation of Tokyo called ‘MeeToo’.
It was a lesson in Japanese culture, mannerisms, personalities and behaviours.
Japanese did not like the orientation part of Second Life and were quickly put off. The first company built an alternative that would suit Japanese rather than US sensibilities.
The answer has been to mimic online the most detailed of Japanese habits, from how they greet and how they gesture, to recreate in.
Can an email-prompted web-based e-learning platform aimed at undergraduates in the UK with moderate to persistent asthma improve compliance to their prescribed preventer drugs to 80%?

Fig. 1 Preventer, Reliever and volumetric. With good adherence the ‘brown one’ is taken as prescribed and the ‘blue one’ rarely needed. With poor adherence there is no brown on and there is dependence on the blue one. In this example a QVAR easibreather and a Venotlin inhaler. Mine.
By presenting these ideas here I asking for support on how to make this research happen.
The medical profession is replacing the term ‘adherence’ with the term ‘compliance’. This reflects the desire to encourage self-management of prescribed drugs in concordance with health care providers (HCPs). For the purposes of this paper the terms should be considered interchangeable.
Asthma is a chronic and complex condition affecting the lungs that can be managed but not cured. (NHS Choices, 2013) (See Appendix 1 for a definition of ‘moderate to persistent asthma’). The World Health Organisation estimates that 300 million people globally are asthmatic (Web, 2001) while in the UK in 2010 5.4 million people were receiving treatment for asthma and there were 1,143 deaths. (Asthma, UK. 2013) An estimated 75% of hospital admissions for asthma are avoidable and as many as 90% of the deaths are preventable. (Asthma, UK. 2013) 80% compliance is the minimal level required for treatment to be effective (Lasmar et al., 2009).
Research construct
Asthmatics form a heterogeneous group that shows great diversity of triggers, effective medication, management strategies and outcomes. Research clusters asthmatics into four to six groups based on how they present and the drug regime they are on (Webb, 2011). Isolating a participant’s conditions and being confident that their medication is correct will be a challenge. For this reason, thorough in-depth interviews with participants, potentially with an HCP present, will be vital in order to set a benchmark.
A team at Harvard Medical School designed Qstream, the proposed e-learning platform (Kerfoot et al., 2008). Qstream (Fig.1.) takes its approach from an understanding of Ebbinghaus (Ebbinghaus, 1913) and how we forget and remember to provide a spaced-learning response that uses a combination of email alerts and interactive content to build knowledge. Its use has been researched with junior doctors in relation to their formal medical training and assessment (Kerfoot et al., 2008; Kerfoot et al., 2012) and in applied settings with healthcare practitioners to support informed decision-making. (Kerfoot et al., 2010)
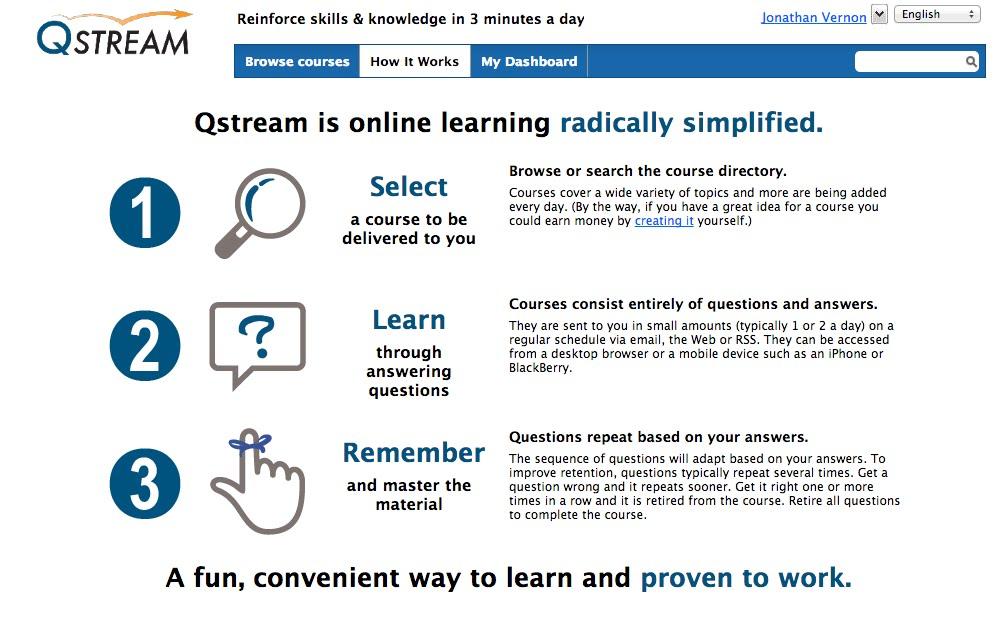
Fig.1. Screengrab from Qstream homepage. (www.qstream.com)
On the basis of their research, Dr B Price Kerfoot says that ‘educational games work’ (Kerfoot et al., 2008. Kerfoot suggests that the next step is to use this approach with patients and ‘clinical decisions of greater complexity’ Kerfoot (2010:477). Research using Qstream involving people with chronic illnesses is planned to take place in North America in the Fall of 2013 (Vernon and Kerfoot, 2013).
What is the problem?
Too many people with a chronic illness, such as asthma, fail to take their medication as prescribed (Royal Pharmaceutical Society (RPS) of Great Britain, 1997; Hayes et al., 1979). This can lead to an exacerbation of the disease, risks hospitalization and even death. Non-compliancy rates are between 10-60% (Cochrane, 1992. Rand,1994), 30–50% (Horne, 1999), 50% (Di Matteo, Giordani, Lepper & Croghan, 2001; Kyngas, 2007 in Wales et al., 2011:148).
Reasons for non-compliance include medication side effects, expense of treatment, personal value judgments or religious or cultural beliefs about the proposed treatment, age–related debility, not having an action plan prescribed by an HCP, the patient not following the adequate treatment prescribed (Cerveri et al., (1999:288) or the presence of a mental disorder (e.g., schizophrenia, personality disorder). American Psychiatric Association [DSM-5], (2013:726).
What is the opportunity?
According to McGavock et al., (1996) efforts to improve compliance have been unsuccessful; it is hoped that efforts using e-learning will be successful. The healthcare community – manufacturers, prescribers and frontline carers, recognise that education offers a way to reduce hospital admissions and deaths (Cerveri et al.,1999:288). The opportunity exists to increase compliance to 80% and therefore improve the health of millions of people with asthma.
A variety of programmes have tested a potential solution to non-adherence. (Byer & Myers, 2000; Hand, 1998; Tettersell, 1993), while Hacihasanoğlu and Goözuöm (2011) showed that patient education on medication adherence is effective. A variety of studies on e-learning in healthcare have used emails linked to multiple-choice questions and answers to improve patients’ knowledge and behaviours (Volpp et al. 2009; Kato et al. 2008).
The hypothesis
The hypothesis is that as a result of greater compliance through a ‘spaced learning’ e-learning education programme, non-compliant moderately persistent asthmatics will show changes in measurements of their illness and changes in their medication beliefs. (Based on Petrie et al., 2012:76).
Desired outcomes / results
Having completed a programme of e-learning using Qstream people with moderate to persistent asthma who had been noncompliant (under 80% compliant) should show changes in their illness and medication beliefs, improved compliance to their preventer inhaler and measured improvement across a range of physiological measures. (Based on Petrie et al., 2012:76) As a result of what they learn, the research will address patient perceptions, such as beliefs (Horne & Weinman, 2002), worries about long term use of steroids (Apter et al., 2003), fears and other concerns (Kaptein, Klok, Moss-Morrs & Brand, 2010). For example, 28% of asthma patients think that drugs are bad and not necessary while 12% think that drugs may not be not bad but aren’t necessary. Cerveri et al., (1999:292).
Achieving a reasonable level of compliance with treatment regimes has been shown to improve the health outcomes of patients undergoing treatment and reduce demands on health resources (Bender, Milgrom, Wamboldt & Rand, 2000; Dunbar-Jacob, Burke & Puczynski, 1995).
The long-term and broader opportunity exists to reduce hospitalizations, reduce costs, improve and extend lives.
Learning Theories
The learning theories that form the basis of Qstream are behaviourist (Skinner, 1974) and cognitive (Wenger, 1987; Hutchins, 1993; Anderson, 1983; Piaget, 1952) with problem solving, explanations and re-combinations. In line with this behaviourist approach early versions of Qstream worked best in formal learning contexts, for example first year medical students needing to pass an exam on anatomy. (Kerfoot et al., 2008) and practical clinical guidelines (Kerfoot et al., 2009). By complementing traditional medical training, with clear goals and the motivation to pass, the attraction of the platform are clear in this context. This stimulus-response approach, builds on the work of Ebbinghaus (1913) (Fig. 2)
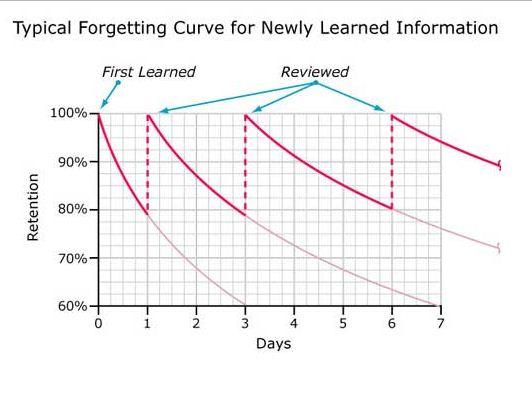
Fig. 2. A typical forgetting curve for newly learned information. After Ebbinghaus (1913)
Through association, the learner takes a number of steps to build a composite skill. (Skinner, 1984; Gagné, 1985) (Fig.3) An accurate reproduction of knowledge can be assessed or demonstrated in drill and practice.
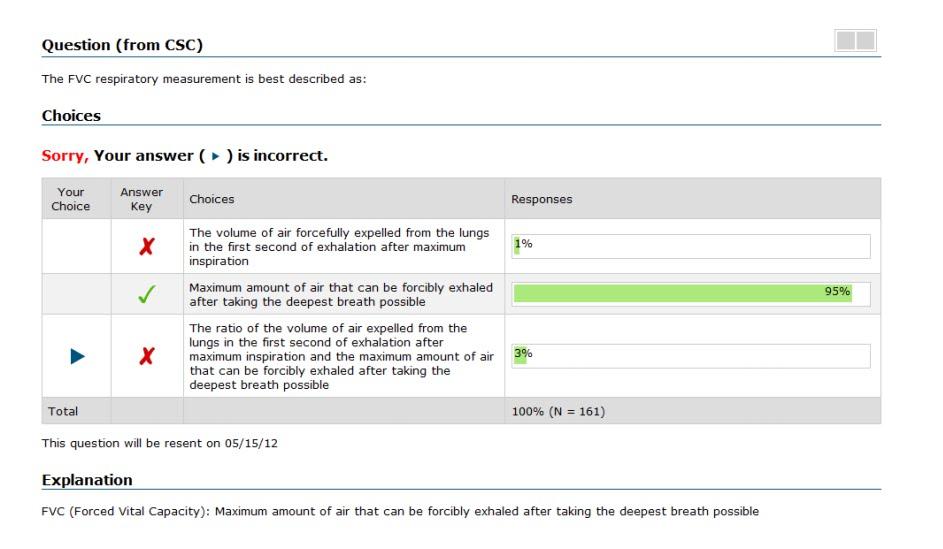
Fig.3. Screengrab from Qstream showing how a participant receives feedback on their response to a multiple-choice question.
Later and current versions of Qstream include components of peer competition, participant interaction and collaboration. This constructivist approach takes the view that learners build their own structures (Piaget, 1954). It also suites task orientated learning (Bruner, 1993) and assimilative learning. This constructed and socio-constructed approach to learning is less suited to assessment simply by looking at exam grades, therefore in-depth interviews or comprehensive self-reporting surveys are required to elicit what took place and the level of knowledge attained especially as evidence of learning by people with asthma won’t be elicited through formal assessment.
Why undergraduates?
The research shows that younger asthma patients in the age 14-25 years are less likely to use their preventer medication than older patients (Diette et al., 1999; Legorreta et al., 1998), which makes ‘young people an important group to target for improving adherence and reducing their underuse of preventer-inhaler corticosteroids’, (Pertie et al., 2012:75). For this reason, and to exploit study parameters of population size and geography, a university undergraduate population is proposed.
METHODOLOGY/METHODS
A mixed-method approach will be adopted with qualitative and quantitative components. In-depth pre and post intervention interviews will form the qualitative element, while the quantitative component will be based on several hundred student participants taking part in a randomized controlled trial and use analytics generated by the Qstream platform. The aim is to interview approximately 30 students in-depth within the parameters of a single university. For example, Adams, Pill & Jones, (1997) favoured in depth interviews with a carefully selected and eligible number of patients before and after intervention. For quantitative analysis the far larger pool of participants will be drawn from a UK wide undergraduate student population using platforms such as The Student Room (www.thestudentroom.com. The Student Room, 2013) and Asthma UK to recruit participants. According to Kerfoot & Baker (2012) an individual randomized control trial is preferable were there is a large sample size. Extending to a sample of four UK universities might increase the potential number of participants to 9000+ (See Appendix 2). Self-reporting screening would be used to ensure that only those in the desired group took part.
Based on UK statistics on asthma in the population, it can be calculated that at, for example, the University of Southampton from a total undergraduate population of 17,000 there are likely to be between 485 and 586 students with moderate to severe asthma. (This intentionally excludes those likely to have a mild form of the disease, and those with a profoundly severe form of the condition). (See Appendix 2 for break down of likely respondents). Asthma UK (2013) suggests that amongst asthmatics 48% consider themselves to be at risk. If this percentage of potential participants volunteered then the starting population for the proposed research is likely to be around 250. It is reasonable to suggest that by working with four different universities of a similar size the total population for a randomized control trial would increase to 1,000.
Identifying those who are moderate to severe asthmatics and agreeing criteria has confounded asthma studies in the past, therefore great care will be required to set parameters, the simplest being that where an asthmatic has been prescribed only two medications, a preventer inhaler (known as the ‘brown one’) and the reliever inhaler (the ‘blue one’) that their condition is considered to be ‘moderate to severe’.
Having a sound basis for giving a person’s baseline, for both compliance and knowledge of asthma and how it is treated, will indicate if an improvement in adherence has been made and whether this e-learning approach has been effective.
To have a physical measure you can audit the prescriptions issued or weigh the inhalers to establish how much has been expelled, however Spector (1985) found cases of both miss-application and trial firing. A blood test is definitive, but this could only be carried out by an HCP. The alternative is to ask patients how they got on, however patients are thought to overestimate their actual drug use by between 30 and 50% (Spector, 1985; Sacket and Snow, 1979). In the case of people with asthma, Horn (1992:126) found that 11% who claimed to have inhaled salbutamol in the preceding four hours had no detectable drug in their urine.
Whilst therefore there are advantages in conducting interviews, patients are giving a subjective measure of their treatment compliance (Sawyer, Rosier and Phelan, 1995). This method suffers from being the most inaccurate of any available (Horn, 1999:126), however the alternative requires a series of tests that need to be administered by an HCP.
This ethnographic investigation would be open and exploratory (RPS, 1997). A system of meanings would be taken either from transcripts (Scherman and Löwhagen, 2004:4) or preferably from audio recordings as current best practice in medical market research favours working from the audio as nuances of meaning are more likely to be apparent (Kazmer & Xie, 2008).
Given the complexity of influencing compliance and the desire to use this as a measure of effective learning, structured and semi-structured in depth interviews will take place. In addition physiological improvements to lung functionality need to be measured for a sample of the participants to offer an objective indicator that a change of behaviour has occurred.
Other influences on outcomes that should be revealed in a semi-structured interview include issues of identity in relation to learning (Kirkup, 2001; and Hughes, 2007) and motivation, what Resnik (2008) describes as ‘passion based learning’.
The text from these interviews will be analysed for clusters of meaning, aiming to pick out nuanced responses, potentially from video but at least from audio recording of interviews (Kazmer & Xie, 2008), which according to Webb (2011) is preferable to working from text alone
The aim would be to reveal the experiences of those interviewed and so come to a view of ‘understandings and misunderstandings’ about their condition, the role their prescribed ‘preventer’ medication plays and the value of Qstream.
Qstream offers a variety of ways to monitor and measure activity on the platform (fig. 4) . This is how data and metadata from several hundred participants would be analysed. (Appendix 3 lists the affordances of using a Qstream private site)
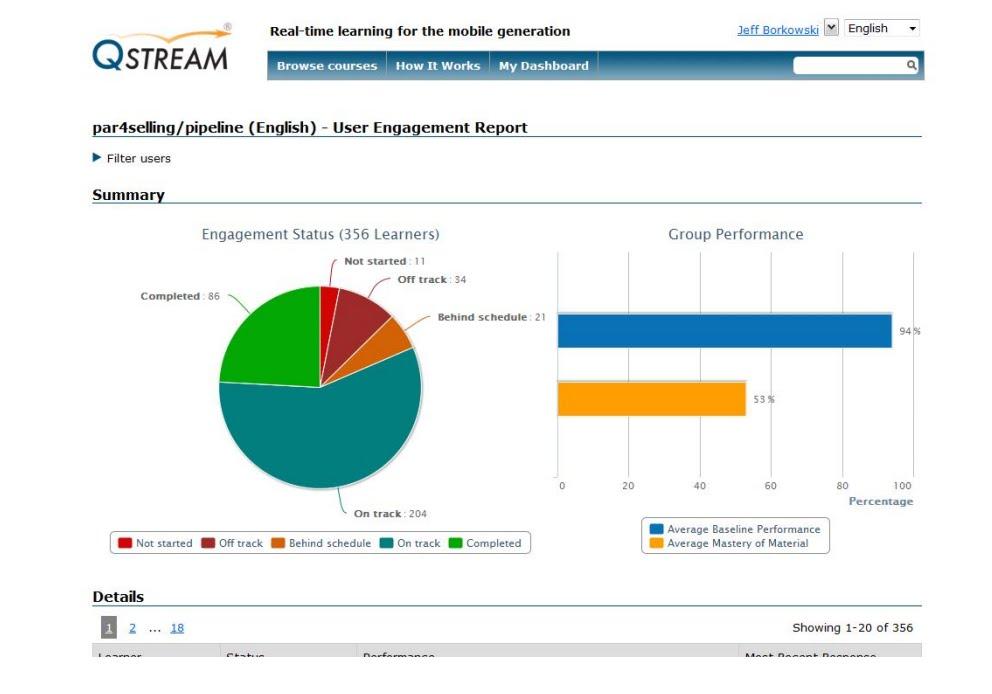
Fig. 4. Screengrab showing example of analytics available on a group of 356 learners.
TIME LINE CHART
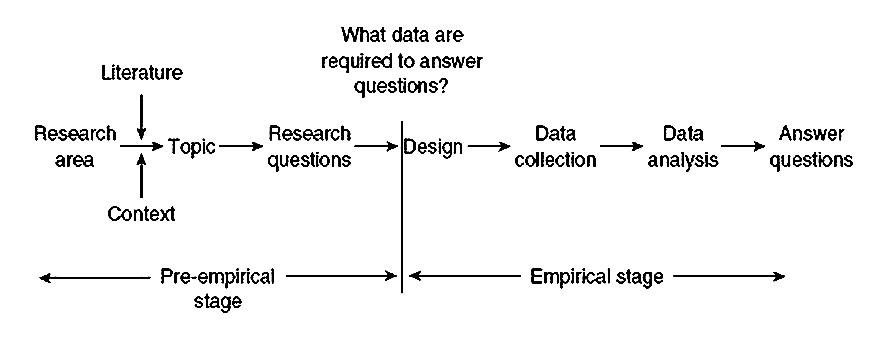
Fig. 5. Simplified model of research. Punch (2006: KL 487 )
Eligibility for interviews and physiological testing would be based on patients with the indicated symptoms though excluding patients with serious social problems and severe learning difficulties. (Franklin et al., 2006)
Aim to recruit 30+ students for in-depth interviews and <1000 for a randomized controlled trial using the Qstream platform. Confirm participants, ensure that they understand the terms and nature of the research and request that they read and agree to these and that participation is voluntary, information will be confidential and their written consent is required. Invite all or some to complete either an asthma Journal or, as they have been shown to be effective, an audio log. Patient-reported outcomes would help us understand the impact of drugs on patients’ lives and activities. “Are patients really doing better? Can they sleep through the night rather than waking up with a sense of shortness of breath?” Bohen (2013: 863)
Pre-Qstream Interviews
Run Qstream e-learning programme for 12 weeks
Post-Qstream Interviews
Analyse data and metadata generated by the Qstream platform
Write up and report findings. Follow up a year later to see if the impact of the learning is maintained over time through changing behaviours. |
Limitations
No study of a therapeutic regime can be considered fully valid without some documentation of whether the patients took their treatment. Horn (1992:127) Establishing valid data on whether people take their medication as prescribed will be a challenge.
No single method of assessment of compliance with (anti-asthma) therapy is ideal nor does any one method give a full picture of the pattern of compliance. Usually the chosen method(s) will require to be validated specifically for the particular circumstances under investigation.
An issue arises with using an Internet and mobile alert system where potentially limited or broken Internet access or paid-for Wi-Fi impinges on the student’s access to the resources. Care will be taken both over how content is scripted and produced, as well as securing a robust platform. Kerfoot and Baker (2012:13) had problems in relation to: ‘server errors’, ‘attrition’ (Kerfoot & Baker, 2012:4), ‘fatigue’ (Kerfoot et al., 2010) and technical hitches due to spam blockers (Shaw et al., 2011) as well as the challenging nature of the content. (In Vernon, 2013)
It is also reasonable to suggest that those who are noncompliant to regularly taking their prescribed medicine could also be ‘noncompliant’ to the features of Qstream – a twice or thrice weekly prompt to take a few minutes to answer some questions.
A UK license for up to 1,000 participants to use the Qstream platform is $15,000 per annum.
In research carried out by ZoRA et al. (1989). Only 1 in 17 diary sheets completed by asthmatic children (under age 14) were accurate to within 10% of the number of puffs used. Whilst the participants in this research are older, any completion of a dairy sheet will include errors and inaccuracies.
Overestimation in self-reporting is well known and probably due to a desire to please. (Cochrane, 1995. Cochrane 1998)
Failure of a therapeutic regime can only be ascribed to poor compliance if appropriate drugs are being prescribed in adequate dosage that historically has tended not to be the situation in the management of asthma. (Horn, 1992:127)
The population using the Internet is diverse. This impacts on research in relation to access and having a representative group of participants. (Eynon, 2009). The use of Qstream in a student population favours use of a mobile device for ease of response to email prompts. It is suggested that 53.7% of people in the UK will be using smartphones by 2014 with those aged 18-25 by far the largest group followed by teenagers (New Media Trend Watch, 2013) whilst it is estimated that nearly 38% will have tablets by this time. (eMarketer, 2013).
Ethics
For ethical reasons an institutional review board would be approached for approval to perform this study. (Kerfoot & Baker, 2012:2) (In Vernon, 2013)
-
A standardized form will be used to obtain informed consent from participants.
-
Well Being, confidentiality and anonymity will be stressed.
-
Rights will be clearly explained
-
The personal safety of those conducting the research will be considered.
-
Conflicts of Interest will be declared, for example, Dr Kerfoot is on the board of Qstream.
-
Unintended consequences will be considered.
-
People have to have the freedom to make mistakes in relation how they elect to adhere, or not, to the prescription drugs they are prescribed. Mental Healthcare Act.
Validity and reliability
If one hope is to correlate a physiological change with improved knowledge an array of factors need to be isolated and measured. Data from both a qualitative and a quantitative approach, the clusters of issues and ideas from analysing what is said in pre and post interviews and the activity on the Qstream platform will offer some indication of what is taking place and why.
Implications for future policies, practice and further research
1) Socio-constructed learning and connectivism
It is further hypothesized that effective compliance is most likely to be achieved where in addition to the patient, the related HCPs engage in the proposed e-learning programme. Social interaction has an important role to play in learning. (Vygotsky, 1978) Donath (2002) shows how through exchanging information a person gains recognition and that social learning of this kind provides affiliation. This suggests value in having HCPs, even family, especially parents and guardians, of younger people with asthma taking part in a Qstream learning programme and exploiting how we connect in networks (Kit Yee et al., 2011) Wang (2008:05) considers the importance in learning of both the student and instructor. HCPs would play the role of ‘intermediaries’ (Laurillard, 1993).
This not only invokes ideas of values relating to communities of practice (Lave and Wenger, 1991) but also, in our digital age, to ‘connectivism’ (Siemens, 2006; Calvani, 2009: de Waard, 2011) – where ‘nodes of readily available information’ are linked to and shared between learners. (Edudemic, 2013) The asthmatic as a learner can question their own knowledge and understanding by connecting with others, as part of a ‘community of practice’ (Lave and Wenger, 1991), from the periphery (Brown, 2002; Brown, 2007) and vicariously (Cox, 2006). Connecting with other people with asthmatics online is supported by the Asthma UK website (Asthma UK, 2013)
2) Use of narrative and creative content
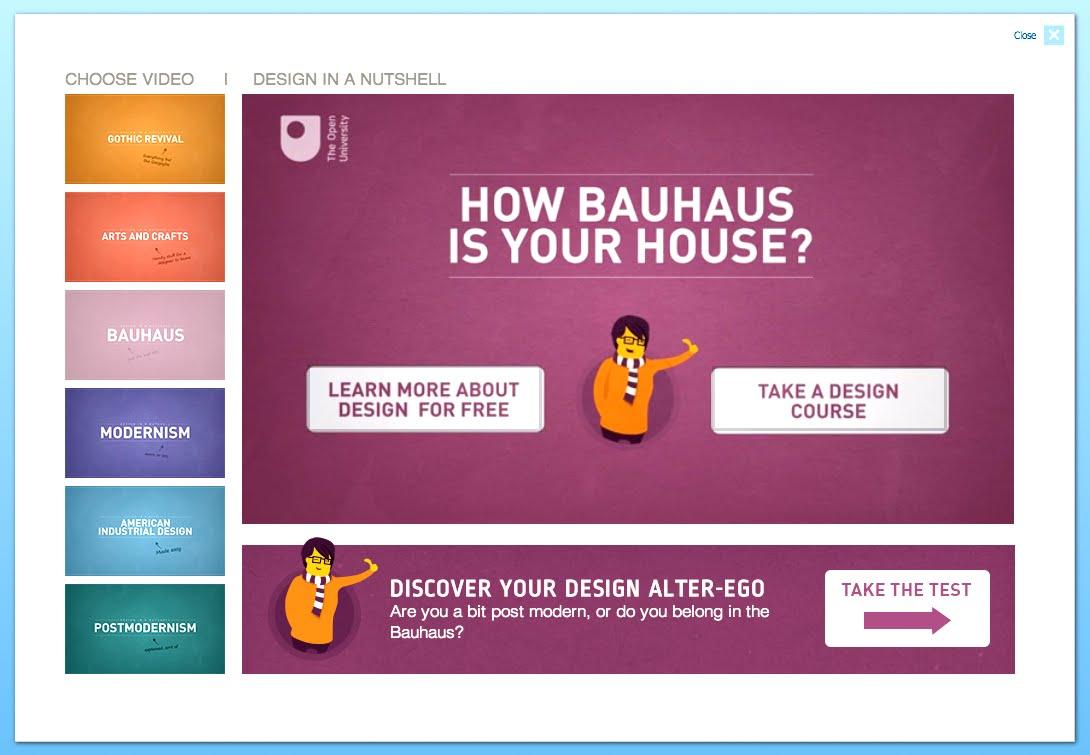
Fig. 5 Screengrab introducing a series of animated videos on design. Open Learn (2013)
The quality and style of scriptwriting using the Qstream platform will impact on effectiveness. (Laurillard, 2000 and Jewell and Hooper, 2011) understand the role of narrative in learning. Resnik and Chang (2008) talk about the need for e-learning to be self-revealing, pleasurable and fun, with a ‘low threshold and high ceiling, supporting collaboration, plugins and making it iterative’ and ‘tinkerable’. The Open University, through Open Learn, often use rich video content to engage audiences, for example with a series of short video in ‘Design in a nutshell’. (Open Learn, 2013)
3) Further personalisation of e-learning
Intelligent Web pages that can adapt themselves to a person’s linguistic and other competence are examples of more ambitious applications that we might look forward to in coming decades. (Hara et al., 2006:352)
4) Extend duration of study period
This study would initially be restricted to a single term or academic year, though it could be extended, for example, to include first year undergraduates through the 3 to 4 year duration of their undergraduate studies. Ostojic et al., (2005) carried out a 4-month trial, whilst trials run by Kerfoot (2008-2012) have run for as long as 45 weeks.
5) Include other chronic illnesses:
Allergic rhinitis is comorbid with asthma (Bousquet at al., 2013) warranting its inclusion in future research alongside studies on asthma. Other chronic illnesses that may benefit from Qstream’s use by patients includes diabetes, epilepsy, Parkinson’s and Alzheimer’s.
6) Consider ‘Big Data’, Web 2.0, Pedagogy 2.0
There is the potential of automatic real-time data gathering relating to inhaler use with a microchip and the use of wearable technology even an ingestible smart pill (Engineer Online 2012; Arnold, 2013) in medicine. Supported by enhanced patient knowledge of their illness. Armed with this data, analysed automatically, and read by the patient or an HCP, the drug regimen and response to it is closely monitored. Such patient analytics are akin to student performance analytics (Koller, 2012) providing HCPS and educators with the potential for gathering and analysing data and metadata from hundreds of thousands of participants.
Conclusion
The opportunity exists to develop an e-learning programme that change lives – that improves the health of those with moderate to persistent asthma. Research suggests that greater knowledge and understanding of a chronic medical condition and personal medical and lifestyle responses and self-management improves compliance. However, the way the illness presents are complex, the triggers and symptoms vary greatly. The approach suggested here also offers the chance to establish if learning brings about a change in behaviour that can be measured in a physiological response – improved lung function and the role an e-learning platform can play. In due course, if a reasonable percentage of the 300+ million asthmatics who are online engage with an e-learning programme such as this significant insights and improvements to health can be made.
REFERENCES
Adams, S., Pill, R., Jones, A. (1997) Medication, chronic illness and identity: the perspective of people with asthma. Soc Sci Med 1997; 45:189-201
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (Revised 5th ed.). Washington, DC: Author.
Arnold, M (2013), ‘A VIEW TO A PILL. (cover story)’, Medical Marketing & Media, 48, 6, pp. 26-30, Business Source Complete, EBSCOhost, viewed 26 June 2013.
Asthma UK (2013) Asthma facts and FAQs. http://www.asthma.org.uk/asthma-facts-and-statistics (Accessed 23rd June 2013)
Bohen, S (2010) Sean Bohen, senior vice president of early development at Genentech (in Smith, B 2010. The Future of Pharma)
Bousquet, J, Khaltaev, N, Cruz, A, Denburg, J, Fokkens, W, Togias, A, Zuberbier, T, Baena-Cagnani, C, Canonica, G, Van Weel, C, Agache, I, Aït-Khaled, N, Bachert, C, Blaiss, M, Bonini, S, Boulet, L, Bousquet, P, Camargos, P, Carlsen, K, & Chen, Y 2008, ‘Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN’, Allergy, 63, pp. 8-160, Academic Search Complete, EBSCOhost, (Accessed 19 June 2013).
Brown, J.S. (2002) The Social Life of Information
Brown, J.S. (2007) October 2007 webcast:http://stadium.open.ac.uk/stadia/preview.php?whichevent=1063&s=31
Calvani, A. (2009). Connectivism: new paradigm or fascinating pot-pourri?. Journal of E-learning and Knowledge Society, 4(1).
Cerveri, I ; Locatelli, F ; Zoia, MC ; Corsico, A ; Accordini , S ; de Marco, R. (1999) International variations in asthma treatment compliance – The results of the European Community Respiratory Health Survey (ECRHS) EUROPEAN RESPIRATORY JOURNAL Volume: 14 Issue: 2 Pages: 288-294 DOI: 10.1034/j.1399-3003.1999.14b09.x Published: AUG 1999 (Accessed 21st June 2013)
Cox, R. (2006) Vicarious Learning and Case-based Teaching of Clinical Reasoning Skills (2004–2006) [online], http://www.tlrp.org/proj/phase111/cox.htm (Accessed 25 June 2013).
de Waard, I. (2011). Explore a new learning frontier: MOOCs. Retrieved from Learning Solutions Magazine website: http://bit. ly/mSi4q
Dukes, DE 2001, ‘What You Should Know about Direct-to-Consumer Advertising of Prescription Drugs’, Defense Counsel Journal, 68, 1, p. 36, Business Source Complete, EBSCOhost, (Accessed 24 June 2013).
Ebbinghaus, M (1913) Memory: A contribution to experimental psychology. (translated by H. A. Ruger and Clara E. Bussenius) 1913, (New York: Teachers College Press),
Edudemic (2013) A simple guide to 4 complex learning theories. http://www.edudemic.com/2012/12/a-simple-guide-to-4-complex-learning-theories/ (Accessed 23 June 2013)
E-Learning Council (2013) Overcoming the Ebbinhause Curve – How we soon forget. http://www.elearningcouncil.com/content/overcoming-ebbinghaus-curve-how-soon-we-forget. (Accessed 23 June 2012)
E-Marketer (2013) UK Tablet use sees robust growth. http://www.emarketer.com/Article/UK-Tablet-Use-Sees-Robust-Growth/1009857 (Accessed 23 June 2013)
Engineer Online (2012) ‘Smart pill containing microchip tracks adherence to medication’ 2012, Engineer (Online Edition), p. 12, Business Source Complete, EBSCOhost, (Accessed 26 June 2013).
Hammersley, M. (1992) What’s Wrong with Ethnography. London: Routledge.
Hayes, R.B., Taylor, D.W., Sacket, D.L. (1979) Compliance in health care. Baltimore: John Hopkins University Press.
Horne, R., & Weinman, J. (2002). Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychology and Health, 17, 17–32. doi:10.1080/08870440290001502
Hughes, G. (2007) ‘Diversity, identity and belonging in e-learning communities: some theories and paradoxes’, Teaching in Higher Education, vol. 12, no. 5, pp. 709-720.
(access 24 June 2013)
Inkpen, K.M. (2000) Designing Handheld Technologies for Kids, Personal Technologies, 3(1-2): 81-9.
Kerfoot, B.P., Armstrong E.G., O’Sullivan P.N. (2008) Interactive spaced education to teach the physical examination: a randomized controlled trial. J Gen Intern Med 2008;23:973–978.
Kerfoot, B.P. (2009) Learning benefits of on-line spaced education persist for 2 years. J Urol 2009;181:2671–2673.
Kerfoot, B.P, Kearney MC, Connelly D, Ritchey ML. (2009) Interactive spaced education to assess and improve knowledge of clinical practice guidelines: a randomized controlled trial. Ann Surg 2009;249:744–749.
Kerfoot, B.P, Lawler EV, Sokolovskaya G, et al. (2010) Durable improvements in prostate cancer screening from online spaced education a randomized controlled trial. Am J Prev Med 2010;39:472– 478.
Kerfoot, B.P., Baker, H., (2012) An Online Spaced-Education Game for Global Continuing Medical Education: A Randomized Trial. Annals of Surgery Volume 256, Number 1, July 2012. pp.1227-1232 www.annalsofsurgery.com
Kerfoot, B.P., Baker, H., Pangaro, L., Agarwal, K., Taffet,G., Mechaber, A.J., Armstrong, E.G. (2012) An Online Spaced-Education Game to Teach and Assess Medical Students: A Multi-Institutional Prospective Trial. Technology and Learning. Academic Medicine, Vol. 87, No. 10 / October 2012 pp. 1443 – 1449
Kirkup, G. (2001) Getting our hands on IT. Gendered inequality in access to ICTs. Conference paper at Gender and Virtual Learning, Hagen, Germany.
Kit Yee, A, Moon, G, Robertson, T, DiCarlo, L, Epstein, M, Weis, S, Reves, R, & Engel, G (2011), ‘Early Clinical Experience With Networked System for Promoting Patient Self-Management’, American Journal Of Managed Care, 17, 7, pp. e277-e287, Academic Search Complete, EBSCOhost, (viewed 19 June 2013).
Koller, D (2012) What we’re learning from online education http://www.youtube.com/watch?feature=player_embedded&v=U6FvJ6jMGHU (Accessed 24 June 2013)
Laurillard, D. (1993). Rethinking university teaching: A framework for the effective use of educational technology.
Lave, J, and Wenger, E. (1991) Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge University Press.
New Media Trend Watch (2013) http://www.newmediatrendwatch.com/markets-by-country/18-uk/154-mobile-devices (Accessed 23 June 2013)
NHS Choices. Health A-Z. Asthma. http://www.nhs.uk/conditions/asthma/Pages/Introduction.aspx (Accessed 23rd June 2013)
Offer, D, Ostrov, E., Howard, K.I. (1977) The Offer Self-Image Questionnaire for Adolescents. A manual, revised. University of Chicago, Illinois.
Open Learn (2013) Design in a nutshell. http://www.open.edu/openlearn/science-maths-technology/engineering-and-technology/design-and-innovation/design/design-nutshell (Accessed 26 June 2013)
Picard, R, Papert, S, Bender, W, Blumberg, B, Breazeal, C, Cavallo, D, Machover, T, Resnick, M, Roy, D, & Strohecker, C (2004) ‘Affective learning – a manifesto’, Bt Technology Journal, 22, 4, pp. 253-269, Science Citation Index, EBSCOhost, (viewed 24 June 2013).
Perlin, K. and Fox, D. (1993) Pad: An Alternative Approach to the Computer Interface, Proceedings of SIGGRAPH ’93:20th Annual Conference on Computer Graphics and Interactive Techniques, 2-6 August 1993, Anaheim, California, USA, 93:57-64.
Petrie K.J., Perry, K., Broadbend, E., Wienman, J (2012) A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication’.
Punch, K.F. (2006) 2nd Edition. Developing Effective Research Proposals.
Resnik, M and Chang, A (2008) Tinkering Together: enabling synchronous creativity and distributed collaboration for kids, MAS 712 Technologies for creative learning.
Royal Pharmaceutical Society (RPS) of Great Britain. (1997) From compliance to concordance: achieving shared goals in medicine taking. London: Royal Pharmaceutical Society of Great Britain
Sawyer, S., Rosier, M. J., & Phelan, P. (1995). The self-image of adolescents with cystic fibrosis. Journal of Adolescent Health, 16(3), 204–208.
Sharples, M., Corlett, D. and Westmancot, O. (2002) The design and implementation of a mobile resource, Personal and Ubiquitous Computing, 6: 220-34.
Soloway, E, Norris, C, Blumenfeld, P, Fishman, B, Krajcik, J, & Marx, R 2001, ‘Handheld Devices are Ready-at-Hand’, Communications Of The ACM, 44, 6, pp. 15-20, Business Source Complete, EBSCOhost, (Accessed 24 June 2013).
Stenhouse, L. (1981) ‘What counts as research?’, British Journal of Educational Studies, vol. 29, no. 2, pp. 103
Scherman, M, & Lawhagen, O (2004), ‘Drug compliance and identity: reasons for non-compliance : experiences of medication from persons with asthma/allergy’, Patient Education & Counseling, 54, 1, pp. 3-9, CINAHL, EBSCOhost, (viewed 12 March 2013).
Siemens, G. (2006). Connectivism: Learning theory or pastime of the self-amused.Retrieved February, 2, 2008.
The Student Room (2013) http://www.thestudentroom.co.uk/ (Accessed 26 June 2013)
Vernon, J.F. (2011) Practice-based research in e-learning (H809). Tutor Marked Assignment 1 (TMA01)
Vernon, J.F., and Kerfoot, B.P. (2013) Skype conversation on the use of e-learning in healthcare in relation to people with chronic illnesses. Considered H809 TMA01. (Unrecorded)
Wang, M., Shen, R., Novak D. and Pan, X. (2008) ‘The impact of mobile learning on students’ learning behaviours and performance: report from a large blended classroom’, British Journal of Educational Technology.
Webb, S (2011) ‘Attacks on asthma’, Nature Biotechnology, 29, 10, pp. 860-863, Academic Search Complete, EBSCOhost, (viewed 12 June 2013).
Wokasch, M. (2010) Pharmaplasia. Wokasch Consulting LLC.
APPENDIX ONE
How to define asthma
MODERATE PERSISTENT – IN THE RESEARCH GROUP (aboutasthma.com)
Your asthma severity is classified as moderate persistent asthma when:
With moderate persistent asthma, you will need daily asthma medication with anti-inflammatory properties, as well as a second medication. You are able to gain control of your asthma with two medications, what we call the ‘blue one’ and the ‘brown one’. The brown one, the inhaled steroid, you take a couple of puffs in the morning and a couple at night. The blue one, the reliever, or what in North America they call the ‘rescue’ inhaler, you take as required Source: National Heart, Lung, and Blood Institute. Accessed: May 20, 2010. Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma |
APPENDIX 2
|
% =/-5% too ill to attend ‘profound’ SOTON 17000 undergraduates First years 5,000 – 5,500 |
Total Soton 9.5% |
Total Soton 11.5% |
First Years 9.5% |
First Years 11.5% |
Across4 UK universities |
|
Approx: students with asthma in the undergraduate population |
1,615 |
1,955 |
475 |
575 |
64,500 |
|
Describing themselves as: 41% very mild |
662 |
801 |
195 |
234 |
26,445 |
|
27% mild |
436 |
528 |
128 |
155 |
17,415 |
|
19% moderate |
307 |
371 |
90 |
109 |
12,255 |
|
11% severe (Wales et al., 2011) |
178 |
215 |
52 |
63 |
7,095 |
|
Moderate to severe likely to be: |
485 |
586 |
142 |
172 |
19,350 |
|
48% think they are at risk (Asthma UK) |
232 |
263 |
68 |
82 |
3,405 |
|
53.7% smartphones by 2014
|
125 |
141 |
37 |
44 |
1,829 |
|
less 4% self exclude from digital devices |
120 |
135 |
36 |
42 |
1,756 |
University of Southampton
Of an undergraduate population at the university of Southampton of 17,000 UK asthma statistics (Asthma UK, 2013) would suggest that between 1 in 10 and 1 in 12 are asthmatic (in a school population 1 in 12 has asthma, while there are 1 in 10 in the general population). Of these 5% have severe asthma and are unlikely to be attending university. This would suggest that between 9.5% and 11.5% as asthmatic. So between 1,615 and 1,955 asthmatic, of whom 662 to 801 likely to say that they are very mild and from 436 to 528 mild so have no medication, or a reliever at most (if they’re right). Between 307 and 371 moderate and 178 to 215 severe – so likely to be on a reliever at least at one end of the spectrum and a preventer too towards the more persistent or severe levels. i.e from 485 to 586. Of these 232 to 263 are likely to think they are ‘at risk’ (Asthma UK). Horn (1992) suggests that patients who admit to poor compliance may be more amenable to compliance modifying strategies; EU funded research into asthma has shown a significant willingness of those with this troublesome disease to take part in research (Cerveri et al., 2013) Whilst use of a smartphone does not define a person as digitally literate a self-reporting interview will isolate those who are … which might be, given use of e-learning in higher education, most of this group. A further reduction is given to exclude some who will not use these devices.
Potentially conducted across four universities:
- University of Southampton. 17,000 students.
- City University, Finsbury, London. 17,000 students. Urban
- University of Cumbria in Lancaster and Newton Rigg, Penrith. 10,500 students. Rural
- University of Oxford. 20,000 students.
APPENDIX THREE
Benefits of a private site using Qstream
|
User admin |
Batch invite |
|
Batch enroll |
|
|
History – invite, enroll |
|
|
Delete |
|
|
Email issue mgmt |
|
|
User registration report |
|
|
Access to learner email addresses |
|
Reporting & analytics |
User tagging |
|
Management roles & reporting |
|
|
Management summary engagement emails (weekly) |
|
|
Engagement summary |
|
|
Engagement detail & export |
|
|
Learner performance summary |
|
|
Learner performance detail & export |
|
|
Snapshot analytics |
|
|
Trend analytics |
|
|
Question performance report |
|
|
Question performance answer matrix |
|
|
Question performance analytics |
|
Site admin |
Monitor site activity |
|
Monitor comment activity for site |
|
|
Site branding (logo, tagline, home page, Dashboard, URL) |
|
|
Site localization (site branding translations) |
|
|
Email branding (sender name, organization logo) |
|
|
Private site publishing privileges |
|
Course admin |
Manage comment activity for course |
|
Shut down courses |
|
|
Basic course branding (course logo, course title) |
|
|
Adv course branding (sender name, organization logo) |
|
|
Private course catalog |
|
|
Public course catalog listing |
|
|
Private, closed courses |
|
|
Open enrollment courses |
|
|
Control course ‘operations’ (spacing, locked/unlocked) |
|
|
Completion management (%, certificate, messaging) |
|
|
Assign authors, co-authors |
|
|
Assign moderators |
|
Learner experience |
Customized leaderboard gaming (email display, online display, invid, team, monthly, rollilng) |
|
Localization |
|
|
Mobile |
Native app with notifications |
|
Mobile interface |
|
|
Course authoring |
Course catalog description/listing |
|
4 question types (MC, MCA, T/F, FIB) |
|
|
Preview/validation of questions |
|
|
Security |
Auto login |
|
Data security |
|
Social & collaboration |
Assign course moderator |
|
Learners can post private or public comments |
|
|
Comment management tools |
Picasa Web Galleries – My Master of Arts in Open and Distance Education in 1,790 images
Google offers a myriad of ways to share content, whether images or words, from galleries to entire conversations. with circles and hangouts. Unwittingly I’ve been part of their ‘game’ since the outset, an early adopter of Picasa having migrated from Flickr. I’ve not invited much in the way of sharing though I now have over 175 ‘albums’ some of which contain a thousand images (the album max). I have THREE album galleries of screengrabs and photos, graphic mash-ups and such like spanning the three years and nine months I’ve been on the MA ODE. This current E-learning III album is taking everything from H818. It is in every respect an OpenStudio platform – if I chose to share its contents then people may, with various copyright permissions (creative commons) use and re-use the content – though plenty of it I grab as a personal aid memoir and is therefore of copyrighted material. I make no apologies for whatever copyright permissions I breach and try to avoid breaking OU guidelines and rules otherwise I’d have grabs from Skype and Elluminate sessions in here. The value of these becomes greater over time – it is a short hand back into a topic, and in time, indicative of how swiftly things are moving. These platforms are leaking out into formal learning contexts; there could be a tipping point, where someone or something happens that galvanises massive interest, say the ‘Stephen Fry’ personality of Twitter, or the Arab Spring of Twitter where J K Rowling or Tracey Emin open their galleries to the world. Meanwhile, without meaning to be unnecessarily derogatory, OpenStudio is the ‘sheep pen’ while Picasa Web Galleries or Google Galleries are the ‘market’ – the sheep pen is closed and local, while the market is global, open, virtual, connected and online.
I have THREE e-learning album galleries of screengrabs and photos, graphic mash-ups and such like spanning the three years and nine months I’ve been on the MA ODE.
This current E-learning III album is taking everything from H818. It is in every respect an OpenStudio platform – if I chose to share its contents then people may, with various copyright permissions (creative commons) use and re-use the content – though plenty of it I grab as a personal aid memoir and is therefore of copyrighted material.
The value of these becomes greater over time – it is a short hand back into a topic, and in time, indicative of how swiftly things are moving. These platforms are leaking out into formal learning contexts; there could be a tipping point, where someone or something happens that galvanises massive interest, say the ‘Stephen Fry’ personality of Twitter, or the Arab Spring of Twitter where J K Rowling or Tracey Emin open their galleries to the world. Meanwhile, without meaning to be unnecessarily derogatory, OpenStudio is the ‘sheep pen’ while Picasa Web Galleries or Google Galleries are the ‘market’ – the sheep pen is closed and local, while the market is global, open, virtual, connected and online.
Reflection on a decade of e-learning

Having not taken stock for a while it was refreshing and re-assuring to consider the Open University postgraduate modules that I have taken, though it has taken this long to understand the meaning of a module that is approaching its final ‘presentation’. In some cases a better word for this might be ‘sell by date’ especially with a subject such as ‘e-learning’ as at least three of those listed below were on their final or penultimate presentation and it mattererd – ‘H817:Innovations in e-learning’ wasn’t particularly innovative for someone who had worked in the creation of interactive and online learning. I’m used to and value the amount of background theory, but I still feel that in these ‘H’ modules that form the Master of Arts in Open and Distance Education (MA ODE) is considerably biased towards learning in formal secondary and tertiary education, rather than applied L&D in business which interested me most – indeed I know of two people across these courses who quit early on because they were working in a learning creation position in business and felt the modules were not suitably applied. B822: Creativity, Innovation and Change was the exception as however dated some of the content (video content shot in the mid 1990s that included companies that had long since gone out of business and innovations such as laptops the size of a small trunk with a carrier bag of cables) the activities and theory in relation to innovation were timeless – it was also an MBA module. Any of us who have taken part in or hosted learning in an organisation involving games of some kind would have found B822 familiar – much of it also touched on the kind of creativity used in advertising, marketing, PR, events and communications.
H804: Implementing Online, Open and Distance Learning (2001)
H807: Innovations in Elearning (2010)
H808: The Elearning professional (2010)
H800: Technology enhanced learning: practices and debates (2011)
B822: Creativity, Innovations and Change (2011)
H810: Accessible online learning: supporting disabled students (2012)
H809: Practice-based research in educational technology (2013)
I’m continuing with these modules to demonstrate that the standard I am now able to achieve is sustainable so that working in academia, even studying for a PhD is viable. ‘H819:The Networked Practitioner’ is a new module. Reading through the course notes and first units (it came online today and goes live next week) I can see the care, clarity and thought that has gone into it, as well as the substantial use of a variety of online learning tools for ‘connected’ or ‘networked’ learning … what some might call ‘social learning’ but here has more structure to it that that (parameters, goals, set tools etc:). It is tailored, every step of the way, to the production of a conference piece – there is considerable latitude here, but what is meant that you have a presentation that may be given in a variety of formats featuring a choice of core themes develop through the module but set in your ‘world’ or field of interest or expertise.
A teacher is taught to teach something in class, not simply to teach.
I feel that I have learnt over the last three years how to teach online, but I haven’t developed a subject specialism, prefering to date to behave as if I were in an e-learning agency serving the needs of many, disperate clients. For this module, and potentially for one or two beyond, I hope to develop and demonstrate how the history of the First World War can be taught using e-learning – apt as we approach its centenary. In parallel I will be taking a Masters in British First World War studies with the University of Birmingham. This is also a part-time course, and ostensibly ‘distance learning’ – though in this instance the distance component is handled by my driving to Edgbaston once a month for a day of intensive face to face seminars and tutorials. This in itself will make for a fascinating constrast with the 100% online experience of the Open University.
In the back of my mind, whatever the subject, my interest is in how to address the global problem of there being 123 million people who want to study at university, but only 5 million places. Even if every university modelled itself on the Open University there would still be a massive shortfall – the answer must be in Open Learning that is supported, possibly by a huge cohort of volunteer alumni, as well as qualifying participants as they accumulate credits. Somewhere in here there may be a question for me to address with doctoral research.
It’s disengenious of me to say that I’ve been studying online for a decade.
I did a module in 2001 but did no further online learning in the subsequent decade – though I did qualify as a swimming teacher and coach! The reason for thinking about a decade as a period of time in which to study is that some would say it takes this long to become an expert. This comes from a piece of research carried out at the Berlin Conservatoire in relation to muscians and the years of training and practice they need to put in to get them to the concert hall as a soloist. Actually it wasn’t years so much as tens of thousands of hours required – 40,000 I think it was with kids introdcued to the instrument early and pushed by parents and institutions getting the furthest youngest. Martin Weller, Professor of e-learning, suggests that a decade is still the time scale in which someone might be deemed a ‘digital scholar’. John Seely Brown, who has applied learning and e-learning to business in the US, notably at Xerox’s famous research institute, suggested earlier this year that scholarship or expertise of the kind we are talking about may be achieved in five years because online learning can speed things up. People do take two degrees in tandem if they study online. Is there a fast track to a PhD? My perspective as a parent with teenagers is that they could begin a part-time online degree in their A’ Level year and graduate at the same time as getting their A’ level results or the year after.
What is WebScience?
WebScience is the scientific study i.e. the identity of problems, the formulation of hypotheses and their in depth scrutiny and analysis, written up and published for sharing, discussion and further debate. This should mean publishing findings with the broadest possible variety of audiences in mind not just to the academic community, from whom further research should be expected, building on the work already done, but to other audiences who through the Web or serendipity, would find the work either appealing, appalling or inspiring.
To help with ‘meaning making’ (Conole, 2011) the metaphor I use to describe the Web is to compare it to the earth’s water cycle where the ocean is awash with digital content, and akin to Web 1.0 influenced by currents and tides, then evaporating into the atmosphere where it forms clouds is shared and transformed (Web 2.0) only to fall as precipitation and return to the ocean.
How much the Web conforms or differs from this pattern helps my analysis and comprehension of what is taking place.
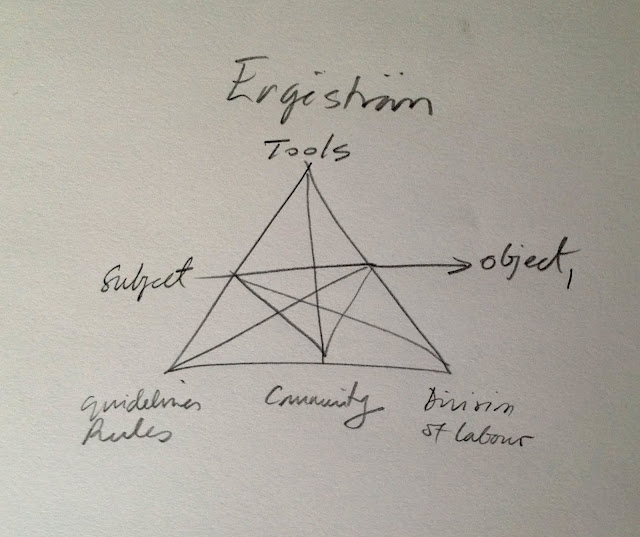
Fig. 1 How we learn behaviourism (Vygotsky) to third generation activity theory (Engeström ) and the World Wide Web. (Doodle by J Vernon, 2013)
A more organic metaphor that places the Web in one context that interests me the workplace is that used by Yrjo Engeström (2008), in which a transmogrification of the model of an Activity System (Fig. 2) becomes like the ‘fingers’ of a funghi. The web after all is alive and growing. Here, an Activity System should be seen not as a static entity, but rather a living and growing thing. KnorrCetina (2003) talks of ‘flow architecture’ and if neither of these concepts ring true for you in then Zerubavel (1997) talks of ‘a mindscape’ while Cussins (1992) talks of ‘cognitive trails’.
Such patterns help describe, explain and predict what is happening in the Web, indeed a third metaphor, building on the ideas of Vannevar Bush from the 1940s, would be to think of the Web as a brain and to draw on lessons being learnt from neuroscience on how complex systems form connections and clusters. In turn, the brain would be an additional important area of study in relation to assistive technologies in relation to chronic illness and memory loss such as with. Alzheimers or Parkinsons.
In relation to WebSciences at the University of Southampton (SOTON) my interest in the iPhD begins with the lofty desire to ‘make a difference’ and to do so drawing on a combination of interests, professional experience, training and study.
It is from a career identifying problems, devising a synopsis, writing treatments, then scripts where amongst a plethora of industry and government an interest in health has developed. This can be pinpointed further to an interest in what role the Web can play in medicine, to inform and support health workers and patients, in particular patients with chronic illnesses such as Alzheimers, Parkinsons, asthma, diabetes and epilepsy.
Focusing even further to one illness and a particular group I have been considering what role e-learning might play to improve adherence to drugs.
I have produced training videos for pharmaceutical companies on the use of preventer inhalers.
My interest with e-learning is to use an inexpensive and readily accessed platform such as Qstream (Kerfoot & Baker, 2012) to deliver appropriate content, including video, through mobile and other devices in order to improve adherence to medication. A literature research has not shown the use of video in this way but there a number of studies where text messaging has been used to improve weight loss (Haapala, 2009), smoking cessation (Rodgers, 2005; Bramley, 2005) and diabetes management (Benhamou, 2007; Cho, 2009; Franklin et al, 2006; Hanauer, 2009; Rami, 2006) which suggests that e-learning initiatives to patients could change behaviours (Cochrane, 1992; Rand, 1994), while emails to multiple-choice questions are used to support medical students. (Kerfoot, 2008, 2009, 2009b, 2010).
A research question I would like to consider is:
‘Can the health of moderate persistent asthmatics aged 14-25 be improved through an e-learning programme that uses targeted emails linked to tailored short videos online (under 90 seconds) in order to achieve adherence to taking their prescribed asthma preventer inhalers to 80% or more?
The appropriateness and relevance to me of such an approach to research is to start with a clearly define problem and place it in a context where scrutiny can occur. In relation to the Web
increasingly the opportunity exists to use and gather ‘big data’, in this instance therefore to have at one level the belief that the globally, all those being treated for asthma form the data set.
Indeed, patients defined as anyone with a chronic illness who should be regularly and consistently taking preventative drugs for a chronic illness would embrace diabetics, those with epilepsy, Parkinson’s and Alzheimers. It is this bigger cohort, and the the role the Web can play to improve the prognosis of those with chronic illnesses that may be the focus of my interest for doctoral research.
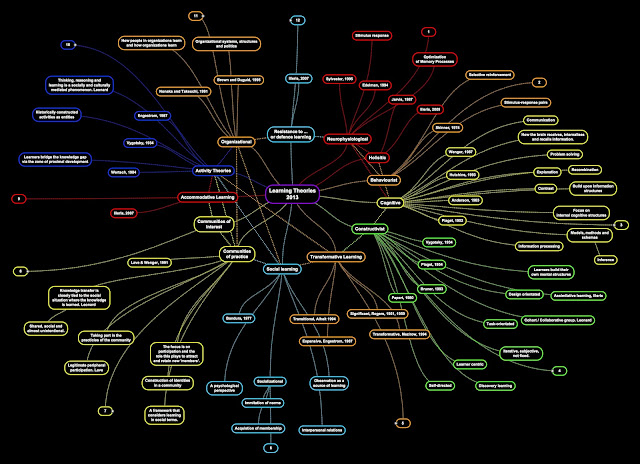
It is vital to understand how people learn insights gained studying for a Masters in Open and Distance Education can in part be summarised in Fig. 6 as from each learning theory comes an appropriate research methodology. How therefore are patients with a chronic illness becoming informed about their condition and why in many cases are they failing to act upon it?
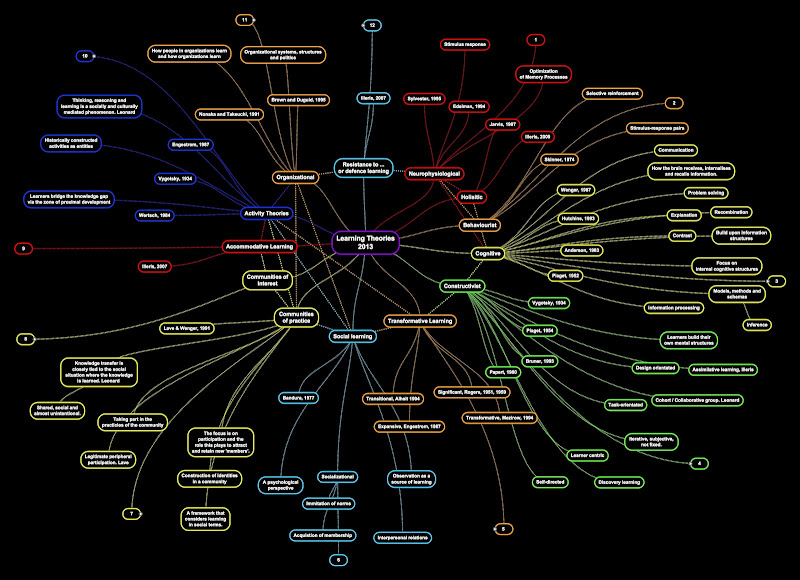
Fig. 2 Learning Theories drawn from multiple sources (Authors given). J Vernon (2013)
REFERENCE
Benhamou PY, Melki V, Boizel R, et al. Oneyear efficacy and safety of web-based follow up using cellular phone in type 1 diabetic patients under insulin pump therapy: the PumpNet Study.
Diabetes Metab. 2007;33(3):220–226.
Bramley D, Riddell T, Whittaker R, et al. (2005) Smoking cessation using mobile phone text messaging is as effective in Maori as non-Maori. N Z Med J. 2005;118(1216):U1494.
Cho JH, Lee HC, Lim DJ, et al. Mobile communication using a mobile phone with a glucometer for glucose control in type 2 patients with diabetes: as effective as an internet-based glucose monitoring system. J Telemed Telecare. 2009;15(2):77–82.
Cochrane, G.M. (1992) Therapeutic compliance in asthma; its magnitude and implications. Eur Respir J 1992;5:122458/
Conole, G (2011) Designing for learning in a digital world. Last accessed 30 May 2013 http://www.slideshare.net/grainne/conolekeynoteicdesept28
Cussins, A. (1992). Content, embodiment and objectivity: The theory of cognitive trails. Mind,
101, 651–688.
Engeström.Y (2008) From Teams to Knots: Activity theoretical studies of Collaboration and Learning at Work. Learning in doing: Social, Cognitive & Computational Perspectives.
Cambridge University Press. Series Editor Emeritus. John Seely Brown.
Franklin, V, Waller, A, Pagliari, C, & Greene, S (2006), ‘A randomized controlled trial of Sweet Talk, a textmessaging system to support young people with diabetes’, Diabetic Medicine, 23, 12, pp. 13321338, Academic Search Complete, EBSCOhost, viewed 16th March 2013
Hanauer DA, Wentzell K, Laffel N, et al. Computerized automated reminder diabetes system
(CARDS): email and SMS cell phone text messaging reminders to support diabetes management. Diabetes Technol Ther. 2009;11(2):99–106.
Haapala I, Barengo NC, Biggs S, et al. (2009) Weight loss by mobile phone: a 1y ear effectiveness study. Public Health Nutr. 2009;12(12):2382–2391.
Kerfoot BP, Armstrong EG, O’Sullivan PN. (2008) Interactive spaced education to teach the physical examination: a randomized controlled trial. J Gen Intern Med 2008;23:973–978. Kerfoot BP. (2009a) Learning benefits of online spaced education persist for 2 years. J Urol 2009;181:2671–2673.
Kerfoot BP, Kearney MC, Connelly D, Ritchey ML. (2009b) Interactive spaced education to assess and improve knowledge of clinical practice guidelines: a randomized controlled trial. Ann
Surg 2009;249:744–749.
Kerfoot BP, Lawler EV, Sokolovskaya G, et al. (2010) Durable improvements in prostate cancer screening from online spaced education a randomized controlled trial. Am J Prev Med 2010;39:472– 478.
Kerfoot, BP., Baker, H., (2012) An Online SpacedEducation Game for Global Continuing Medical Education: A Randomized Trial. Annals of Surgery Volume 256, Number 1, July 2012. pp.12271232 http://www.annalsofsurgery.com
Kerfoot, BP., Baker, H., Pangaro, L., Agarwal, K., Taffet,G., Mechaber, A.J., Armstrong, E.G. (2012) An Online Spaced Education Game to Teach and Assess Medical Students: A Multi-national Prospective Trial. Technology and Learning. Academic Medicine, Vol. 87, No. 10 / October 2012 pp. 1443 -1449
KnorrCetina, K. (2003). From pipes to scopes: The flow architecture of financial markets. Distinktion, 7, 7–23.
Rand, C.S., Wise, R.A. (1994) Measuring adherence to asthma medication regimens. Am J Respir Crit Care Med 1994; 149:6976
Rami B, Popow C, Horn W, et al. (2006) Telemedical support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur J Pediatr. 2006;165(10):701–705.
Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005;14(4):255–261.
Zerubavel, E. (1997). Social mindscapes: An invitation to cognitive sociology. Cambridge, MA: Harvard University Press.
Related articles
- Living with Chronic Illness Changes Your Life (theadventuresofarthritisnfibromyalgia.wordpress.com)
- The Ingredients of being chronically ill (brainlesionandme.com)
- An A to Z of chronic illness: Part 5 (brainlesionandme.com)
13 E-learning theories
|
Associative/ Behaviourist approaches
|
Design principles
|
|
Looking for observable behaviour
|
Explicitly mentioning course outcomes
|
|
Behavioural objectives
|
Ability to test achievement of learning outcomes
|
|
Instructional Systems Design (ISD)
|
Decomposing learning into small chunks
|
|
Routines of organised activity
|
|
|
Learning hierarchies (controversial!)
|
Sequencing learning materials with increasing complexity
|
|
Giving direct feedback on learning
|
|
|
Individualized learning trajectories
|
|
|
Cognitive psychology (constructivism)
|
|
|
Types of memory (sensory – short term – long term)
|
Maximize sensations: strategic screen layout
|
|
Research on memory, perception, reasoning, concept formation.
|
Maximize sensations: well-paced information
|
|
Learning is active
|
Maximize sensations: highlighting main elements
|
|
Learning is individual (knowledge construction)
|
Relate difficulty level to cognitive level of learner: providing links to easier and more advanced resources
|
|
Use of comparative advance organizers
|
|
|
Use of conceptual models
|
|
|
Importance of prior knowledge structures
|
Pre-instructional & prerequisite questions
|
|
Experimentation toward discovery of broad principles
|
|
|
Promote deep processing
|
Use of information maps zooming in/ out
|
|
Cognitive Apprenticeship (Brown et al, 1989)
|
Interactive environments for construction of understanding
|
|
Metacognition (reflection, self-regulation)
|
Relate to real-life (apply, analyse, synthesize)
|
|
Learning styles (controversial!)
|
Address various learning styles
|
|
Cognitive styles
|
Let students prepare a journal
|
|
Dual coding theory
|
Use both visual information and text
|
|
Motivate learners (ARCS model)
|
Use techniques to catch attention, explain relevance, build confidence and increase satisfaction
|
|
Situated learning (constructivism)
|
|
|
Personal knowledge construction
|
Personal meaning to learning
|
|
Situated learning: motivation
|
Relate to real life (relevance)
|
|
Holistic/ Systemic approaches
|
Conduct research on internet
|
|
Build confidence with learners
|
|
|
Identity development
|
Use of first-hand information (not filtered by instructor)
|
|
Communities of Practice (Lave & Wenger)
|
Collaborative activities
|
|
Zone of Proximal Development (Vygotsky)
|
Fostering the growth of learning communities
|
|
Learning as act of participation
|
Legitimate (peripheral) practice, apprenticeships
|
|
Lifelong learning
|
Authentic learning and assessment tasks
|
|
Connectivism
|
|
|
Information explosion
|
Digital literacies
|
|
Learning in network environment
|
Keep up-to-date in field
|
|
Knowledge base
|
Multi-channel learning
|
|
Distributed learning
|
Build diversity, openness in learning (different opinions), autonomy
|
|
Personal Learning Environment
|
self-directed learning, just-in-time |
Constructivism – Jonassen et al 1999
Social Constructions – Vygotsky 1986
Activity Theory – Engeström et al 1999
Experiational Learning – Kolb 1984
Instructional Design – Gagné et al 2004
Networked and collaborative work – McConnell 2000
Learning Design Jochems et al 2004
Primary: presenting information
Secondary: active learning and feedback
Tertiary: dialogue and new learning.
Related articles
- Module 3 – Learning and Technology Theories Reflection (natalieedit202.wordpress.com)
- Learning Theory (downes.ca)
- Learning Theory – What are the established learning theories? (miracletrain2013.wordpress.com)
- Learning Theories and Technology (daniellegroten.wordpress.com)
- Connectivism: A Learning Theory for the Digital Age (gamedynamics.wordpress.com)
- Social Constructivism (s4323697.wordpress.com)
Methodological Innovation
From the Oxford Internet Institute
Methodological innovation is vital given the changing nature of the Internet and advances in ICTs which both necessitate and facilitate the development of new techniques.
OII researchers are developing methodologies such as:
- big data approaches;
- the embedding of ICT s for real time observation of social phenomenon;
- webmetric techniques for observing the underlying structure of the web presence of social institutions;
- artificial intelligence design;
- experimental research;
- on-line action research;
- content analysis;
- investigation of virtual environments;
- and online survey research.
The five current research foci examine the role of the Internet and other ICTs in:
- government and democracy: where ICT s offer significant opportunities for restructuring practices and institutions, for example in the management and delivery of government services and the functioning of governance processes
- research and learning: focusing on the use and impact of ICTs within academic and research communities and the social and institutional contexts in which this takes place
- everyday life and work: covering the role of the Internet and other ICTs in personal interactions in the household, the arts, and entertainment, and the needs of individuals and the wider community in work, social relationships, leisure, and activities in other arenas that bring society online
- shaping the Internet: how rapidly developing ICTs are liberated or constrained, including how the Internet itself is governed.
- network economy: how ICTs reshape business models, markets and economic development.
